

Contributions
Abstract: EP995
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Multiple Myeloma (MM) disease course is a succession of remissions and relapses, which define lines of treatment. For each line, several regimens can be used. Although guidelines provide recommendations on the disease management, real world data are missing to describe which regimens are used in the daily practice. Regarding recent changes due to the introduction of new drugs (e.g., daratumumab, carfilzomib and ixazomib), an accurate and updated overview of MM treatment management is needed. This study provides a comprehensive overview of these recent changes based on the nationwide French National Health Insurance (NHI) databases, called SNDS (“Système National des Données de Santé”). These databases include hospital records, primary and secondary care of 66 million people.
Aims
To describe the evolution over time of MM treatment management by line and treatment sequencing in practice in France, in the context of a new therapeutic landscape.
Methods
This is a retrospective observational cohort study including all cases of multiple myeloma from 2014 to 2018 identified through the French NHI databases (SNDS). Cases were detected using a validated algorithm which was expanded to consider recent evolutions of MM therapeutic management. Treatment lines were re-constructed through ATLAS, a published adaptation of the Smith-Waterman alignment sequence algorithm, by scanning day-by-day patient claims. This innovative algorithm gave the temporal flexibility needed, and impossible with a solely rule-based identification, to identify lines considering the possible deviations between theoretical regimens and patient reality, and between reality and claim data. For each year (2014-2018) and for each line, the number and percentage of patients starting a regimen was assessed and protocols detailed.
Results
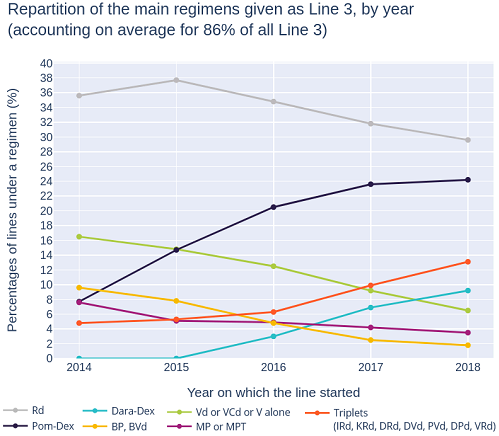
36,208 prevalent patients treated for a MM between 2014 and 2018 were included. As expected, the main regimen for L1 without transplant changed from VMP (2014: 32%) to Rd (2018: 30%), the place of VRd regimen rapidly increased (2017: 4%, 2018: 10%), whereas MPT and MP regimens decreased (together, 2014: 19%, 2018: 4%). For L1 with transplant, VTd remains the main regimen (2014: 59%; 2018: 61%). Same for Rd on L2 and L3 (L2 - 2014: 47%, 2018: 54%; L3 - 2014: 36%; 2018: 30%), although we observed a shifting of some standards from doublet to triplet therapy (IRd, KRd, DRd, DVd, DPd, PVd, and VRd) with the newest drugs, as presented in the attached figure. Moreover, L4+ landscape is broadly evolving with a main regimen changed from Pom-Dex (2014: 21%) to Dara-Dex (2018: 21%). The rapidly acquired place of Pom-Dex in L3 (2018: 24%) can be related to the shift to the use of lenalidomide in earlier lines (L1, L2), hence inducing more lenalidomide-refractory patients. Regarding treatment sequences, the main course of patients having a L4+ in 2018 was as follows: L1 : V-based regimen (VMP for non-transplant ; VTd for transplant); L2: Rd; L3: Pom-Dex; L4+: Dara-Dex. All these results will be updated (Q2-2021) and presented with 2019 data.
Conclusion
This study demonstrates the fast evolution of treatment management of MM patients, due to new drug marketing authorizations. The study also showed that real-world data are a powerful tool to study treatment lines at a national scale and lead the way to more precise analyses of optimal therapeutic sequences, including their impact on the overall survival.
Keyword(s): Epidemiology, Multiple myeloma, Treatment
Abstract: EP995
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Multiple Myeloma (MM) disease course is a succession of remissions and relapses, which define lines of treatment. For each line, several regimens can be used. Although guidelines provide recommendations on the disease management, real world data are missing to describe which regimens are used in the daily practice. Regarding recent changes due to the introduction of new drugs (e.g., daratumumab, carfilzomib and ixazomib), an accurate and updated overview of MM treatment management is needed. This study provides a comprehensive overview of these recent changes based on the nationwide French National Health Insurance (NHI) databases, called SNDS (“Système National des Données de Santé”). These databases include hospital records, primary and secondary care of 66 million people.
Aims
To describe the evolution over time of MM treatment management by line and treatment sequencing in practice in France, in the context of a new therapeutic landscape.
Methods
This is a retrospective observational cohort study including all cases of multiple myeloma from 2014 to 2018 identified through the French NHI databases (SNDS). Cases were detected using a validated algorithm which was expanded to consider recent evolutions of MM therapeutic management. Treatment lines were re-constructed through ATLAS, a published adaptation of the Smith-Waterman alignment sequence algorithm, by scanning day-by-day patient claims. This innovative algorithm gave the temporal flexibility needed, and impossible with a solely rule-based identification, to identify lines considering the possible deviations between theoretical regimens and patient reality, and between reality and claim data. For each year (2014-2018) and for each line, the number and percentage of patients starting a regimen was assessed and protocols detailed.
Results
36,208 prevalent patients treated for a MM between 2014 and 2018 were included. As expected, the main regimen for L1 without transplant changed from VMP (2014: 32%) to Rd (2018: 30%), the place of VRd regimen rapidly increased (2017: 4%, 2018: 10%), whereas MPT and MP regimens decreased (together, 2014: 19%, 2018: 4%). For L1 with transplant, VTd remains the main regimen (2014: 59%; 2018: 61%). Same for Rd on L2 and L3 (L2 - 2014: 47%, 2018: 54%; L3 - 2014: 36%; 2018: 30%), although we observed a shifting of some standards from doublet to triplet therapy (IRd, KRd, DRd, DVd, DPd, PVd, and VRd) with the newest drugs, as presented in the attached figure. Moreover, L4+ landscape is broadly evolving with a main regimen changed from Pom-Dex (2014: 21%) to Dara-Dex (2018: 21%). The rapidly acquired place of Pom-Dex in L3 (2018: 24%) can be related to the shift to the use of lenalidomide in earlier lines (L1, L2), hence inducing more lenalidomide-refractory patients. Regarding treatment sequences, the main course of patients having a L4+ in 2018 was as follows: L1 : V-based regimen (VMP for non-transplant ; VTd for transplant); L2: Rd; L3: Pom-Dex; L4+: Dara-Dex. All these results will be updated (Q2-2021) and presented with 2019 data.
Conclusion
This study demonstrates the fast evolution of treatment management of MM patients, due to new drug marketing authorizations. The study also showed that real-world data are a powerful tool to study treatment lines at a national scale and lead the way to more precise analyses of optimal therapeutic sequences, including their impact on the overall survival.
Keyword(s): Epidemiology, Multiple myeloma, Treatment