

Contributions
Abstract: EP950
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Biology & Translational Research
Background
In newly diagnosed as well as in relapsed/refractory multiple myeloma, the anti CD38 monoclonal antibody daratumumab (Dara) has become essential in the therapeutic arsenal. Unfortunately, a subset of patients is not responding to Dara, or is progressing quickly after initiation of therapy. Different characteristics of the disease can be studied to predict and try to understand those response profiles. In addition to clinical markers, we looked at karyotypic and genomic parameters. We have also used plasma cell phenotyping with multiparametric flow cytometry (MFC) on CD200, CD117, CD56, CD38, CD45 and CD27. In particular, CD200 has been shown to be an independent pejorative prognostic factor for progression-free survival in myeloma patients and could play an important role in immunosuppression and regulation of anti-tumor activity.
Aims
Find clinical, karyotypic, genomic or phenotypic predictive markers of response to daratumumab in multiple myeloma.
Methods
We retrospectively included 97 multiple myeloma patients treated with Dara at Montpellier University Hospital. Standard clinical and therapeutic data were collected for all patients. Transcriptomic data were available in 68% of patients, and cytogenetic data in 47.5% of patients. All the patients had MFC data available before treatment with Dara. We collected the expression of CD200, CD117, CD27, CD45, CD56 and the mean fluorescence intensity of CD38 at diagnosis. Patients who obtained at least a partial response were considered as responders.
Results
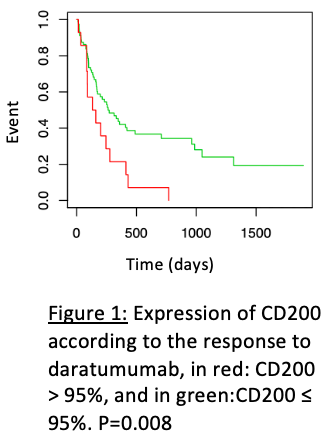
The median age at Dara start was 68 years, and 59.8% of patients were responders versus 39.2% non-responders. The majority of patients were treated in monotherapy (48.5%). The Dara was given in combination with lenalidomide in 23.7% of patients, with bortezomib in 15.5%, with pomalidomide in 5.2% and with both lenalidomide and bortezomib in 3.1%. The median number of prior lines of therapy was 3 [0-7]. As expected, response to Dara was significantly associated with longer PFS (P<0.0001) and OS (P<0.0001). Within the various clinical and therapeutic data, the only significant parameter associate to the presence of response in multivariate analysis was the use of Dara in combination (P=0.03). Of note, complex karyotype was significantly associated with the absence of response to Dara, but only in univariate analysis (probably due to small number of events: 7 patients with complex karyotype). Comparing gene expression profiling (GEP) data of responder (n=24) versus non-responder patients (n=12) using GSEA revealed a significant enrichment in inflammatory response genes, genes encoding extracellular matrix and polycomb PRC2 as well as H3K27me3 target genes. Finally, Maxstat analysis of CD200 expression found that an expression of this protein in more than 95% of plasma cells was significantly associated with the absence of response to Dara (Figure). Similarly, expression of CD27 and CD45 were significantly associated with poor response to Dara. We did not find any significant correlation between Dara response and CD117 expression, CD56 expression nor CD38 mean fluorescence intensity (all patients were CD38 positive).
Conclusion
Overall, our data seem to show that low expression of the checkpoint inhibitor CD200 and enrichment in inflammatory response genes expression is associated with good response to Dara. Further work is ongoing to understand the underlying mechanisms and to determine whether phenotypic or gene expression data could be used as predictive markers of response to Dara.
Keyword(s): Gene expression profile, Monoclonal antibody, Myeloma, Phenotype
Abstract: EP950
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Biology & Translational Research
Background
In newly diagnosed as well as in relapsed/refractory multiple myeloma, the anti CD38 monoclonal antibody daratumumab (Dara) has become essential in the therapeutic arsenal. Unfortunately, a subset of patients is not responding to Dara, or is progressing quickly after initiation of therapy. Different characteristics of the disease can be studied to predict and try to understand those response profiles. In addition to clinical markers, we looked at karyotypic and genomic parameters. We have also used plasma cell phenotyping with multiparametric flow cytometry (MFC) on CD200, CD117, CD56, CD38, CD45 and CD27. In particular, CD200 has been shown to be an independent pejorative prognostic factor for progression-free survival in myeloma patients and could play an important role in immunosuppression and regulation of anti-tumor activity.
Aims
Find clinical, karyotypic, genomic or phenotypic predictive markers of response to daratumumab in multiple myeloma.
Methods
We retrospectively included 97 multiple myeloma patients treated with Dara at Montpellier University Hospital. Standard clinical and therapeutic data were collected for all patients. Transcriptomic data were available in 68% of patients, and cytogenetic data in 47.5% of patients. All the patients had MFC data available before treatment with Dara. We collected the expression of CD200, CD117, CD27, CD45, CD56 and the mean fluorescence intensity of CD38 at diagnosis. Patients who obtained at least a partial response were considered as responders.
Results
The median age at Dara start was 68 years, and 59.8% of patients were responders versus 39.2% non-responders. The majority of patients were treated in monotherapy (48.5%). The Dara was given in combination with lenalidomide in 23.7% of patients, with bortezomib in 15.5%, with pomalidomide in 5.2% and with both lenalidomide and bortezomib in 3.1%. The median number of prior lines of therapy was 3 [0-7]. As expected, response to Dara was significantly associated with longer PFS (P<0.0001) and OS (P<0.0001). Within the various clinical and therapeutic data, the only significant parameter associate to the presence of response in multivariate analysis was the use of Dara in combination (P=0.03). Of note, complex karyotype was significantly associated with the absence of response to Dara, but only in univariate analysis (probably due to small number of events: 7 patients with complex karyotype). Comparing gene expression profiling (GEP) data of responder (n=24) versus non-responder patients (n=12) using GSEA revealed a significant enrichment in inflammatory response genes, genes encoding extracellular matrix and polycomb PRC2 as well as H3K27me3 target genes. Finally, Maxstat analysis of CD200 expression found that an expression of this protein in more than 95% of plasma cells was significantly associated with the absence of response to Dara (Figure). Similarly, expression of CD27 and CD45 were significantly associated with poor response to Dara. We did not find any significant correlation between Dara response and CD117 expression, CD56 expression nor CD38 mean fluorescence intensity (all patients were CD38 positive).
Conclusion
Overall, our data seem to show that low expression of the checkpoint inhibitor CD200 and enrichment in inflammatory response genes expression is associated with good response to Dara. Further work is ongoing to understand the underlying mechanisms and to determine whether phenotypic or gene expression data could be used as predictive markers of response to Dara.
Keyword(s): Gene expression profile, Monoclonal antibody, Myeloma, Phenotype