

Contributions
Abstract: EP881
Type: E-Poster Presentation
Session title: Lymphoma Biology & Translational Research
Background
Angioimmunoblastic T cell lymphoma (AITL) is an aggressive malignancy with poor response to conventional chemotherapy. AITL is a subcategory of peripheral T cell lymphomas. Despite the approval of CD30 directed antibody drug conjugate- Brentuximab vedotin (BV), the prognostic role of CD30 in AITL is unknown.
Aims
The main aim of this study was to study the prognostic significance of CD30 expression in AITLThe main aim of the single instituition retrospective study was to elucidate the prognostic implications of CD30 in AITL.
Methods
We analyzed patients newly diagnosed with AITL at our institution between 2000 and 2020. Along with CD30 receptor testing, variables such as date of diagnosis included age, gender, stage, LDH level, platelets, hemoglobin, bone marrow involvement, and EBV receptor positivity were collected. Treatment and progression data including response to frontline therapy, presence of consolidation stem cell transplant (SCT), and usage of brentuximab-based treatment. Endpoints were progression free survival (PFS) and OS; Univariate (UVA) and multivariate (MVA) Cox proportional hazard models were used to determine the significance of variables at diagnosis on PFS and OS.
Results
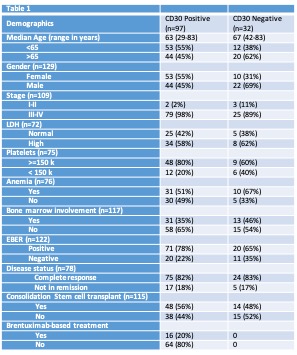
Out of the 295 individuals diagnosed with AITL,129 patients with CD30 testing who had response and survival data were included. This group had a median age of 65 (range 29-83) years and male predominance (51%) were identified. Table 1 summarizes patient and disease characteristics. Median follow up time was 40 (range 2-137) months, with three-year PFS and OS of 48% and 23% respectively. Sixty-seven individuals died within the first three years of the study. The 3-year OS is 46% in CD30+ individuals, and 55% in those who are CD30- (p=0.578). PFS is 20% in CD30+ individuals, and 29% in those who are CD30- (p-0.675). The variables included in Table 1 were assessed using UVA. Achieving Complete remission (CR) following frontline therapy (p=<0.0001) and consolidation with SCT (p=0.0428) were significantly associated with improved PFS. For OS, age <65 (p=0.0129), female gender (p=0.0437), and SCT (p=0.0003) were statistically associated with improved survival. CD30 and variables with p-value <0.15 were included in MVA. For PFS, achieving CR to frontline therapy (reference, complete remission), (HR 2.987, 95% CI: 1.524-5.855, p=0.0014) and consolidation with SCT (reference, SCT) (HR 2.036, 95% CI: 1.208-3.432, p=0.0076) were associated with better PFS. For OS, age >65 (HR 3.131, 95%CI: 1.545-6.344, p=0.0015), BM involvement (HR 2.134, 95% CI: 1.151-3.956, p=0.0161), incomplete remission (HR 2.208, 95% CI: 1-4.876, p=0.0499), male gender (HR 0.367, 95% CI: 0.199-0.678, p=0.0014), no SCT (HR 4.085, 95% CI: 2.119-7.872, p=<0.0001) and positive CD30 (reference, positive CD30) (HR 0.322, 95% CI: 0.158-0.656, p=0.0018) were associated with inferior OS.
Conclusion
Age <65, achieving CR to induction treatment, and upfront SCT proved to be strong predictors of improved OS. In our cohort, only 20% of our patients received BV; nevertheless, unlike previous studies, individuals with CD30 positivity did not trend towards better OS. Therefore, additional work on CD30 biology in AITL is warranted.
Keyword(s): CD30, Survival prediction, T cell lymphoma
Abstract: EP881
Type: E-Poster Presentation
Session title: Lymphoma Biology & Translational Research
Background
Angioimmunoblastic T cell lymphoma (AITL) is an aggressive malignancy with poor response to conventional chemotherapy. AITL is a subcategory of peripheral T cell lymphomas. Despite the approval of CD30 directed antibody drug conjugate- Brentuximab vedotin (BV), the prognostic role of CD30 in AITL is unknown.
Aims
The main aim of this study was to study the prognostic significance of CD30 expression in AITLThe main aim of the single instituition retrospective study was to elucidate the prognostic implications of CD30 in AITL.
Methods
We analyzed patients newly diagnosed with AITL at our institution between 2000 and 2020. Along with CD30 receptor testing, variables such as date of diagnosis included age, gender, stage, LDH level, platelets, hemoglobin, bone marrow involvement, and EBV receptor positivity were collected. Treatment and progression data including response to frontline therapy, presence of consolidation stem cell transplant (SCT), and usage of brentuximab-based treatment. Endpoints were progression free survival (PFS) and OS; Univariate (UVA) and multivariate (MVA) Cox proportional hazard models were used to determine the significance of variables at diagnosis on PFS and OS.
Results
Out of the 295 individuals diagnosed with AITL,129 patients with CD30 testing who had response and survival data were included. This group had a median age of 65 (range 29-83) years and male predominance (51%) were identified. Table 1 summarizes patient and disease characteristics. Median follow up time was 40 (range 2-137) months, with three-year PFS and OS of 48% and 23% respectively. Sixty-seven individuals died within the first three years of the study. The 3-year OS is 46% in CD30+ individuals, and 55% in those who are CD30- (p=0.578). PFS is 20% in CD30+ individuals, and 29% in those who are CD30- (p-0.675). The variables included in Table 1 were assessed using UVA. Achieving Complete remission (CR) following frontline therapy (p=<0.0001) and consolidation with SCT (p=0.0428) were significantly associated with improved PFS. For OS, age <65 (p=0.0129), female gender (p=0.0437), and SCT (p=0.0003) were statistically associated with improved survival. CD30 and variables with p-value <0.15 were included in MVA. For PFS, achieving CR to frontline therapy (reference, complete remission), (HR 2.987, 95% CI: 1.524-5.855, p=0.0014) and consolidation with SCT (reference, SCT) (HR 2.036, 95% CI: 1.208-3.432, p=0.0076) were associated with better PFS. For OS, age >65 (HR 3.131, 95%CI: 1.545-6.344, p=0.0015), BM involvement (HR 2.134, 95% CI: 1.151-3.956, p=0.0161), incomplete remission (HR 2.208, 95% CI: 1-4.876, p=0.0499), male gender (HR 0.367, 95% CI: 0.199-0.678, p=0.0014), no SCT (HR 4.085, 95% CI: 2.119-7.872, p=<0.0001) and positive CD30 (reference, positive CD30) (HR 0.322, 95% CI: 0.158-0.656, p=0.0018) were associated with inferior OS.
Conclusion
Age <65, achieving CR to induction treatment, and upfront SCT proved to be strong predictors of improved OS. In our cohort, only 20% of our patients received BV; nevertheless, unlike previous studies, individuals with CD30 positivity did not trend towards better OS. Therefore, additional work on CD30 biology in AITL is warranted.
Keyword(s): CD30, Survival prediction, T cell lymphoma