

Contributions
Abstract: EP804
Type: E-Poster Presentation
Session title: Indolent and mantle-cell non-Hodgkin lymphoma - Clinical
Background
Population-based studies in LPL/WM are limited. Nevertheless, these studies revealed that the introduction of rituximab improved the population-level survival of LPL/WM patients across all age groups. The improved survival necessitates measures that capture the prognosis for long-term LPL/WM survivors because survival estimates measured from diagnosis can be rather discouraging due to patients who die within the first years post-diagnosis. Conditional relative survival (CRS) is a concept that refers to the probability of survival—corrected for the life expectancy in the general population—after having survived from a specified time since diagnosis. Studies on CRS in LPL/WM lack to inform long-term LPL/WM survivors about their prognosis at a specified time since diagnosis.
Aims
This nationwide, population-based study examined up-to-date estimates of 5-year relative survival (RS) at diagnosis and for each year survived up to 15 years post-diagnosis among LPL/WM patients in the Netherlands.
Methods
All patients diagnosed with LPL/WM between 1989-2018—with follow-up for survival until December 31, 2019—were selected from the Netherlands Cancer Registry. RS was calculated to estimate disease-specific survival. RS is defined as the ratio of the observed to expected survival, of which the latter is matched to the patient by age, sex, and calendar year. We calculated 5-year RS at diagnosis and 5-year CRS for each additional year survived up to fifteen years after diagnosis, conditional on being alive at the beginning of that year. Up-to-date survival probabilities for patients diagnosed during 1989-2018 who were alive between the follow-up interval of 2008-2019, were generated using the hybrid approach. These survival probabilities can be interpreted as the predicted survival probabilities for patients diagnosed during 2008-2019. Survival statistics were computed for the overall cohort and according to sex and age at diagnosis (≤65 and >65). Survival differences between the point estimates were assessed by 95% CI overlap.
Results
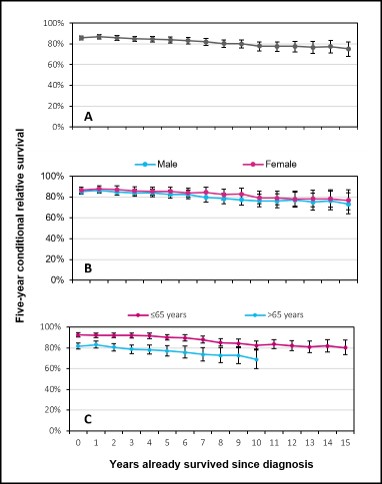
A total of 6,234 LPL/WM patients (median age, 70 years; and 61% males) were diagnosed in the Netherlands during 1989-2018, of whom 4,296 (69%) were at risk under the hybrid approach. The overall 5-year RS measured from diagnosis was 86% (95% CI, 84%>88%) and gradually decreased with additional years survived to 75% (95% CI, 68%>82%) at 15 years post-diagnosis (Fig. A). This trend was emulated according to sex, with no sex differential in survival over time (Fig. B). However, there were significant differences in 5-year RS at diagnosis with increasing age, namely 93% (95% CI, 91%>95%), and 82% (95% CI, 79%>85%) across the age groups, respectively (Fig. C). Five-year CRS decreased with each additional year survived among patients aged ≤65 and >65 years at diagnosis. Consequently, the age-related survival gap persisted during the follow-up period.
Conclusion
This study highlights that contemporary diagnosed LPL/WM patients, as compared to the general population, continue to experience excess mortality regardless of having survived up to 15 years post-diagnosis. This gradual increase in excess mortality might result from the incurable nature of this disease characterized by multiple relapses throughout the disease course. CRS estimates offer LPL/WM patients information about their survival expectations with each year survived post-diagnosis and provides means to physicians to tailor surveillance and follow-up activities. Our study results touch upon the need for novel treatment strategies to reduce short- and long-term excess mortality in LPL/WM patients.
Keyword(s): Lymphoplasmacytic lymphoma, Population, Survival, Waldenstrom's macroglobulinemia
Abstract: EP804
Type: E-Poster Presentation
Session title: Indolent and mantle-cell non-Hodgkin lymphoma - Clinical
Background
Population-based studies in LPL/WM are limited. Nevertheless, these studies revealed that the introduction of rituximab improved the population-level survival of LPL/WM patients across all age groups. The improved survival necessitates measures that capture the prognosis for long-term LPL/WM survivors because survival estimates measured from diagnosis can be rather discouraging due to patients who die within the first years post-diagnosis. Conditional relative survival (CRS) is a concept that refers to the probability of survival—corrected for the life expectancy in the general population—after having survived from a specified time since diagnosis. Studies on CRS in LPL/WM lack to inform long-term LPL/WM survivors about their prognosis at a specified time since diagnosis.
Aims
This nationwide, population-based study examined up-to-date estimates of 5-year relative survival (RS) at diagnosis and for each year survived up to 15 years post-diagnosis among LPL/WM patients in the Netherlands.
Methods
All patients diagnosed with LPL/WM between 1989-2018—with follow-up for survival until December 31, 2019—were selected from the Netherlands Cancer Registry. RS was calculated to estimate disease-specific survival. RS is defined as the ratio of the observed to expected survival, of which the latter is matched to the patient by age, sex, and calendar year. We calculated 5-year RS at diagnosis and 5-year CRS for each additional year survived up to fifteen years after diagnosis, conditional on being alive at the beginning of that year. Up-to-date survival probabilities for patients diagnosed during 1989-2018 who were alive between the follow-up interval of 2008-2019, were generated using the hybrid approach. These survival probabilities can be interpreted as the predicted survival probabilities for patients diagnosed during 2008-2019. Survival statistics were computed for the overall cohort and according to sex and age at diagnosis (≤65 and >65). Survival differences between the point estimates were assessed by 95% CI overlap.
Results
A total of 6,234 LPL/WM patients (median age, 70 years; and 61% males) were diagnosed in the Netherlands during 1989-2018, of whom 4,296 (69%) were at risk under the hybrid approach. The overall 5-year RS measured from diagnosis was 86% (95% CI, 84%>88%) and gradually decreased with additional years survived to 75% (95% CI, 68%>82%) at 15 years post-diagnosis (Fig. A). This trend was emulated according to sex, with no sex differential in survival over time (Fig. B). However, there were significant differences in 5-year RS at diagnosis with increasing age, namely 93% (95% CI, 91%>95%), and 82% (95% CI, 79%>85%) across the age groups, respectively (Fig. C). Five-year CRS decreased with each additional year survived among patients aged ≤65 and >65 years at diagnosis. Consequently, the age-related survival gap persisted during the follow-up period.
Conclusion
This study highlights that contemporary diagnosed LPL/WM patients, as compared to the general population, continue to experience excess mortality regardless of having survived up to 15 years post-diagnosis. This gradual increase in excess mortality might result from the incurable nature of this disease characterized by multiple relapses throughout the disease course. CRS estimates offer LPL/WM patients information about their survival expectations with each year survived post-diagnosis and provides means to physicians to tailor surveillance and follow-up activities. Our study results touch upon the need for novel treatment strategies to reduce short- and long-term excess mortality in LPL/WM patients.
Keyword(s): Lymphoplasmacytic lymphoma, Population, Survival, Waldenstrom's macroglobulinemia