

Contributions
Abstract: EP797
Type: E-Poster Presentation
Session title: Indolent and mantle-cell non-Hodgkin lymphoma - Clinical
Background
Mantle Cell lymphoma (MCL) represents 3-10% of all non-Hodgkin B-cell lymphoma with a third of new diagnoses affecting patients (pts) aged >75 years. Although the treatment options for MCL have increased over the last years with the introduction of Bruton Kinase Inhibitors (BTKi), for older and unfit pts, treatment options are limited. Practice across the UK varies with regimens such as attenuated R-CHOP, R-CVP, attenuated R-Bendamustine (R-B), R-Chlorambucil (R-CHL) used. Outcomes in this population are not fully characterised.
Aims
This study aims to identify treatment pattens and outcomes of the most commonly used attenuated and low intensity regimens used in pts with newly diagnosed MCL unfit for standard chemoimmunotherapy (i.e. full dose R-CHOP or R-B).
Methods
Data were retrospectively collected across 19 centres in the UK and Ireland between 1/1/2010 and 31/11/2020. All pts who were ineligible for standard regimens and had received at least 1 dose of an attenuated or low intensity regimen. Baseline characteristics, treatment characteristics and toxicity data were collected. Progression free survival (PFS) and overall survival (OS) were calculated using standard Kaplan-Meier analysis. Univariable and multivariable Cox regression analysis (MVA) was used to examine the associations between baseline factors, regimens, PFS and OS.
Results
95 pts (attenuated RCHOP n=22, attenuated R-B n=24, R-CHL n=30, R-CVP, n=19) were analysed. Median age was 79 years (range:58-89) with baseline ECOG of 0, 1 and ≥2 for 22.1, 41.1% and 36.8% respectively. 50% were ≥80 years and median CIRS-G score was 6 (range:0-24). 93% had stage III-IV disease with 91% presenting with high MIPIb or MIPI score. 14.5% had blastoid morphology. Pts receiving R-CHL had higher age, with worse ECOG and along with those receiving R-CVP had greater CIRS-G than the other groups.
Overall response rate (ORR) for the whole cohort was 72% with a median duration of response (DoR) of 19.1 months (95% CI 12.9-25.4). Numerically higher ORR and DoR were observed in attenuated R-B and R-CHOP (83.3%, 33.8 months and 82%, 22 months). 60 pts progressed with 47 receiving further treatment including 36 receiving Ibrutinib.
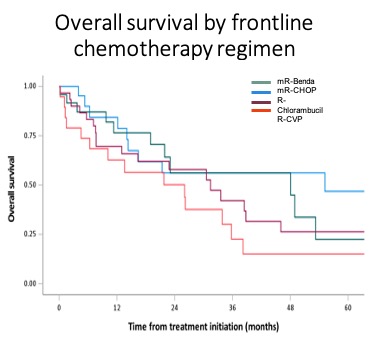
Median PFS for all pts was 15 months (95% CI:8.7-21.2) and median OS was 31.4 months (95% CI:19.7-43.2). The median PFS and OS for attenuated R-CHOP pts was 16.7 months (95% CI 9.8-23.7) and 55.2 months (95% CI 1.9-108.4), attenuated R-B pts was 21.9 months (95% CI 0-46.3) and 48.1 months (95% CI 0-109.5), R-CVP pts was 7.4 months (95% CI 0.3-14.5) and 26.1 months (95% CI 2.7-49.4), and R-CHL pts was 12.0 months (95% CI 5.4-18.7) and 31.4 months (95% CI 17.9-45.0) respectively.
By MVA, factors associated with an inferior PFS were bulk (>10cm) (HR:2.05, p=0.04) and blastoid morphology (HR:2.63, p=0.02). Higher treatment intensity (R-CHOP/R-B composite) provided a superior PFS compared with RCVP/R-CHL (MVA HR:0.48, p=0.01). Factors associated with inferior OS by MVA were age (HR:1.06), ECOG performance status (HR:2.50), blastoid morphology (HR:3.12) and POD24 status (HR:4.37).
Conclusion
Overall, PFS and OS following front-line dose attenuated immunochemotherapy is unsatisfactory. POD24 association with worse OS is now validated in elderly frail pts. Outcomes were generally poor, but attenuated R-CHOP or R-B may improve disease control compared to R-CVP or R-CHL. Clinical trials investigating novel agents such as BTK and BCL2 inhibitors in this specific clinical setting are warranted.
Keyword(s): Elderly, Mantle cell lymphoma
Abstract: EP797
Type: E-Poster Presentation
Session title: Indolent and mantle-cell non-Hodgkin lymphoma - Clinical
Background
Mantle Cell lymphoma (MCL) represents 3-10% of all non-Hodgkin B-cell lymphoma with a third of new diagnoses affecting patients (pts) aged >75 years. Although the treatment options for MCL have increased over the last years with the introduction of Bruton Kinase Inhibitors (BTKi), for older and unfit pts, treatment options are limited. Practice across the UK varies with regimens such as attenuated R-CHOP, R-CVP, attenuated R-Bendamustine (R-B), R-Chlorambucil (R-CHL) used. Outcomes in this population are not fully characterised.
Aims
This study aims to identify treatment pattens and outcomes of the most commonly used attenuated and low intensity regimens used in pts with newly diagnosed MCL unfit for standard chemoimmunotherapy (i.e. full dose R-CHOP or R-B).
Methods
Data were retrospectively collected across 19 centres in the UK and Ireland between 1/1/2010 and 31/11/2020. All pts who were ineligible for standard regimens and had received at least 1 dose of an attenuated or low intensity regimen. Baseline characteristics, treatment characteristics and toxicity data were collected. Progression free survival (PFS) and overall survival (OS) were calculated using standard Kaplan-Meier analysis. Univariable and multivariable Cox regression analysis (MVA) was used to examine the associations between baseline factors, regimens, PFS and OS.
Results
95 pts (attenuated RCHOP n=22, attenuated R-B n=24, R-CHL n=30, R-CVP, n=19) were analysed. Median age was 79 years (range:58-89) with baseline ECOG of 0, 1 and ≥2 for 22.1, 41.1% and 36.8% respectively. 50% were ≥80 years and median CIRS-G score was 6 (range:0-24). 93% had stage III-IV disease with 91% presenting with high MIPIb or MIPI score. 14.5% had blastoid morphology. Pts receiving R-CHL had higher age, with worse ECOG and along with those receiving R-CVP had greater CIRS-G than the other groups.
Overall response rate (ORR) for the whole cohort was 72% with a median duration of response (DoR) of 19.1 months (95% CI 12.9-25.4). Numerically higher ORR and DoR were observed in attenuated R-B and R-CHOP (83.3%, 33.8 months and 82%, 22 months). 60 pts progressed with 47 receiving further treatment including 36 receiving Ibrutinib.
Median PFS for all pts was 15 months (95% CI:8.7-21.2) and median OS was 31.4 months (95% CI:19.7-43.2). The median PFS and OS for attenuated R-CHOP pts was 16.7 months (95% CI 9.8-23.7) and 55.2 months (95% CI 1.9-108.4), attenuated R-B pts was 21.9 months (95% CI 0-46.3) and 48.1 months (95% CI 0-109.5), R-CVP pts was 7.4 months (95% CI 0.3-14.5) and 26.1 months (95% CI 2.7-49.4), and R-CHL pts was 12.0 months (95% CI 5.4-18.7) and 31.4 months (95% CI 17.9-45.0) respectively.
By MVA, factors associated with an inferior PFS were bulk (>10cm) (HR:2.05, p=0.04) and blastoid morphology (HR:2.63, p=0.02). Higher treatment intensity (R-CHOP/R-B composite) provided a superior PFS compared with RCVP/R-CHL (MVA HR:0.48, p=0.01). Factors associated with inferior OS by MVA were age (HR:1.06), ECOG performance status (HR:2.50), blastoid morphology (HR:3.12) and POD24 status (HR:4.37).
Conclusion
Overall, PFS and OS following front-line dose attenuated immunochemotherapy is unsatisfactory. POD24 association with worse OS is now validated in elderly frail pts. Outcomes were generally poor, but attenuated R-CHOP or R-B may improve disease control compared to R-CVP or R-CHL. Clinical trials investigating novel agents such as BTK and BCL2 inhibitors in this specific clinical setting are warranted.
Keyword(s): Elderly, Mantle cell lymphoma