

Contributions
Abstract: EP764
Type: E-Poster Presentation
Session title: Hodgkin lymphoma - Clinical
Background
The relative benefit of targeted agents increasingly investigated and applied in relapsed or refractory Hodgkin lymphoma (rrHL) is difficult to estimate due to a lack of randomized trials.
Aims
This retrospective study thus aimed at evaluating disease characteristics, treatment patterns and associated outcomes at first occurrence of rrHL after contemporary first-line treatment.
Methods
We retrospectively identified patients with sufficiently documented first rrHL initially receiving standard of care 1st-line treatment in the GHSG HD13 (early-stage favorable), HD14 (early-stage unfavorable) and HD15 (advanced-stage) trials. We additionally evaluated rrHL patients enrolled in the placebo-controlled randomized GHSG HDR3i trial comparing conventional DHAP vs. everolimus + DHAP salvage therapy prior planned autologous stem-cell transplantation (ASCT). We assessed overall survival (OS) starting with date of 1st rrHL and ending with date of death for any reason and progression free survival (PFS) measured from date of rrHL to second rrHL or death from any reason. Patient, disease and treatment characteristics were analyzed with descriptive statistics and survival endpoints with Kaplan-Meier estimates.
Results
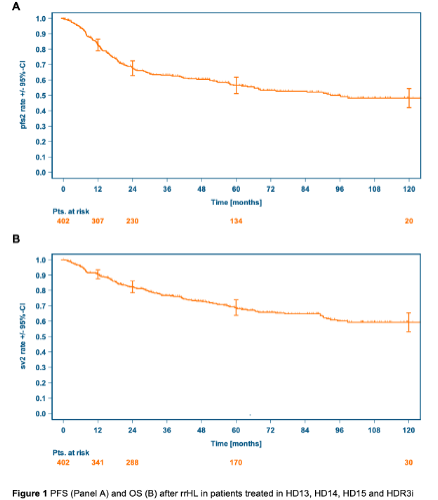
A total of 437 patients with first rrHL (HD13: n=87, HD14: n= 118, HD15: n=188, HDR3i: n=44) were identified. Of these, 402 patients with sufficient documentation and follow-up were assessed with a median age of 37.5 years (18.4-76.8). Time to relapse was ≤12 months in 49% and stage III/IV rrHL present in 52% of patients. High-dose chemotherapy and autologous stem-cell transplantation (ASCT) with and without consolidation was administered in 20% and 52% of patients, respectively. The remaining 111 patients (27%) did not receive ASCT mostly due to insufficient response to salvage chemotherapy, advanced age, localized disease or patients’ preference. Overall, 10-year PFS and OS after first relapse were 48.2% (95% confidence interval CI: 42.0%>54.4%) and 59.3% (95%CI: 53.2%>65.4%), respectively (Figure 1). Patients unsuitable for ASCT had less favorable 10-year PFS (32.5%, 95%CI: 19.1%>45.9%) and OS (41.9%, 95%CI: 28.1%>55.6%). Significantly inferior PFS and OS was also observed in primary refractory patients (10-year PFS 36.0%, 95%CI: 24.2%>47.9%; 10-year OS 44.5%, 95%CI: 31.6%>56.6%) and those with stage IV disease at rrHL (10-year PFS 29.3%, 95%CI: 18.5%>40.9%; 10-year OS 39.6%, 95%CI: 27.9%>51.1%). Outcomes in these higher risk patients appeared more favorable with ASCT than without ASCT.
Conclusion
Our analysis of relapse and treatment patterns after contemporary HL therapy provides a robust benchmark to evaluate novel therapeutic strategies in rrHL. We confirm the curative potential of current rrHL treatments including non-ASCT approaches and roughly 50% of rrHL patients do not experience a consecutive relapse after 2nd-line treatment.
Keyword(s): Hodgkin's lymphoma, Outcome, Relapsed lymphoma, Treatment
Abstract: EP764
Type: E-Poster Presentation
Session title: Hodgkin lymphoma - Clinical
Background
The relative benefit of targeted agents increasingly investigated and applied in relapsed or refractory Hodgkin lymphoma (rrHL) is difficult to estimate due to a lack of randomized trials.
Aims
This retrospective study thus aimed at evaluating disease characteristics, treatment patterns and associated outcomes at first occurrence of rrHL after contemporary first-line treatment.
Methods
We retrospectively identified patients with sufficiently documented first rrHL initially receiving standard of care 1st-line treatment in the GHSG HD13 (early-stage favorable), HD14 (early-stage unfavorable) and HD15 (advanced-stage) trials. We additionally evaluated rrHL patients enrolled in the placebo-controlled randomized GHSG HDR3i trial comparing conventional DHAP vs. everolimus + DHAP salvage therapy prior planned autologous stem-cell transplantation (ASCT). We assessed overall survival (OS) starting with date of 1st rrHL and ending with date of death for any reason and progression free survival (PFS) measured from date of rrHL to second rrHL or death from any reason. Patient, disease and treatment characteristics were analyzed with descriptive statistics and survival endpoints with Kaplan-Meier estimates.
Results
A total of 437 patients with first rrHL (HD13: n=87, HD14: n= 118, HD15: n=188, HDR3i: n=44) were identified. Of these, 402 patients with sufficient documentation and follow-up were assessed with a median age of 37.5 years (18.4-76.8). Time to relapse was ≤12 months in 49% and stage III/IV rrHL present in 52% of patients. High-dose chemotherapy and autologous stem-cell transplantation (ASCT) with and without consolidation was administered in 20% and 52% of patients, respectively. The remaining 111 patients (27%) did not receive ASCT mostly due to insufficient response to salvage chemotherapy, advanced age, localized disease or patients’ preference. Overall, 10-year PFS and OS after first relapse were 48.2% (95% confidence interval CI: 42.0%>54.4%) and 59.3% (95%CI: 53.2%>65.4%), respectively (Figure 1). Patients unsuitable for ASCT had less favorable 10-year PFS (32.5%, 95%CI: 19.1%>45.9%) and OS (41.9%, 95%CI: 28.1%>55.6%). Significantly inferior PFS and OS was also observed in primary refractory patients (10-year PFS 36.0%, 95%CI: 24.2%>47.9%; 10-year OS 44.5%, 95%CI: 31.6%>56.6%) and those with stage IV disease at rrHL (10-year PFS 29.3%, 95%CI: 18.5%>40.9%; 10-year OS 39.6%, 95%CI: 27.9%>51.1%). Outcomes in these higher risk patients appeared more favorable with ASCT than without ASCT.
Conclusion
Our analysis of relapse and treatment patterns after contemporary HL therapy provides a robust benchmark to evaluate novel therapeutic strategies in rrHL. We confirm the curative potential of current rrHL treatments including non-ASCT approaches and roughly 50% of rrHL patients do not experience a consecutive relapse after 2nd-line treatment.
Keyword(s): Hodgkin's lymphoma, Outcome, Relapsed lymphoma, Treatment