

Contributions
Abstract: EP715
Type: E-Poster Presentation
Session title: Enzymopathies, membranopathies and other anemias
Background
Autoimmune haemolytic anaemia (AIHA) is a critical health concern where myriad factors contribute to this autoimmune syndrome. There are no clear recommendations in the latest consensus of AIHA regard the different forms and regimens of corticosteroids in the treatment of the warm type.
Aims
we aim to compare the efficacy and safety of regimens started with intravenous corticosteroids and the regimen of prednisolone alone as first-line strategies for newly diagnosed adult warm AIHA.
Methods
The current study is a single-centre prospective cohort (NCT03269292, Clinical Trials.gov) conducted in a university-affiliated hospital (Assiut University Hospital, Assiut, Egypt). Subjects were enrolled if they have warm AIHA with positive direct antiglobulin (DAT) test either primary or secondary type and their age is more than 18 years. We excluded patients with previously treated AIHA and other types of immune haemolytic anaemia
The patients either administrated oral prednisolone 1mg/kg daily for 3 weeks or started therapy with one of three different regimens for the intravenous corticosteroid therapy: intravenous dexamethasone 40 mg daily for 4 days, Methylprednisolone 1 gram/day for 3 days, or Methylprednisolone 1 gram/day for 5 days then followed by oral prednisolone 1 mg/kg/day for the rest of the 3 weeks. Full clinical evaluation and CBC were done every 3 days for 3 weeks.
Results
156 eligible newly diagnosed AIHA patients were recruited to the cohort and they receive corticosteroids as first line therapy.
The median hemoglobin level recorded at the baseline was significantly higher (p=0.001) in patients started the treatment with prednisolone orally (5.8g/dl) than patients started treatment with intravenous regimens (4.5g/dl). However, the median incremental increase of hemoglobin level from the baseline was significantly higher (p=0.003) in the patients started with intravenous regimens (3.1g/dl) than the other group (2g/dl).
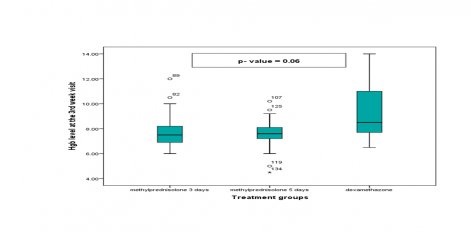
The analysis of the subgroups of patients started with intravenous regimens showed that no significant difference in the hemoglobin level at the baseline between the three treatment regimens (p=0.1). Although there was not any significant difference between these three groups regard the hemoglobin level at the end of the 3rd week but there was a trend to be higher in the dexamethasone group (figure 1).
There was not any significant difference between the regimens started with intravenous crticosteroids and the oral regimen alone as regard the frequency of the adverse events (p=0.3). The adverse events reported were either grade 1 or grade 2 and included hyperglycaemia, hypertensin, muscle weakness, hypokalaemia, abdominal pain and vomiting. They were not associated with long term sequalae or death.
Conclusion
In this study, we prove that regimens started with intravenous corticosteroids therapy are superior to oral regimen as they achieved higher levels of incremental increase in the hemoglobin levels from the baseline without increase of the incidence or increase the severity of the side effects. This is beneficial in cases of acute sever AIHA.
Keyword(s): Autoimmune hemolytic anemia (AIHA)
Abstract: EP715
Type: E-Poster Presentation
Session title: Enzymopathies, membranopathies and other anemias
Background
Autoimmune haemolytic anaemia (AIHA) is a critical health concern where myriad factors contribute to this autoimmune syndrome. There are no clear recommendations in the latest consensus of AIHA regard the different forms and regimens of corticosteroids in the treatment of the warm type.
Aims
we aim to compare the efficacy and safety of regimens started with intravenous corticosteroids and the regimen of prednisolone alone as first-line strategies for newly diagnosed adult warm AIHA.
Methods
The current study is a single-centre prospective cohort (NCT03269292, Clinical Trials.gov) conducted in a university-affiliated hospital (Assiut University Hospital, Assiut, Egypt). Subjects were enrolled if they have warm AIHA with positive direct antiglobulin (DAT) test either primary or secondary type and their age is more than 18 years. We excluded patients with previously treated AIHA and other types of immune haemolytic anaemia
The patients either administrated oral prednisolone 1mg/kg daily for 3 weeks or started therapy with one of three different regimens for the intravenous corticosteroid therapy: intravenous dexamethasone 40 mg daily for 4 days, Methylprednisolone 1 gram/day for 3 days, or Methylprednisolone 1 gram/day for 5 days then followed by oral prednisolone 1 mg/kg/day for the rest of the 3 weeks. Full clinical evaluation and CBC were done every 3 days for 3 weeks.
Results
156 eligible newly diagnosed AIHA patients were recruited to the cohort and they receive corticosteroids as first line therapy.
The median hemoglobin level recorded at the baseline was significantly higher (p=0.001) in patients started the treatment with prednisolone orally (5.8g/dl) than patients started treatment with intravenous regimens (4.5g/dl). However, the median incremental increase of hemoglobin level from the baseline was significantly higher (p=0.003) in the patients started with intravenous regimens (3.1g/dl) than the other group (2g/dl).
The analysis of the subgroups of patients started with intravenous regimens showed that no significant difference in the hemoglobin level at the baseline between the three treatment regimens (p=0.1). Although there was not any significant difference between these three groups regard the hemoglobin level at the end of the 3rd week but there was a trend to be higher in the dexamethasone group (figure 1).
There was not any significant difference between the regimens started with intravenous crticosteroids and the oral regimen alone as regard the frequency of the adverse events (p=0.3). The adverse events reported were either grade 1 or grade 2 and included hyperglycaemia, hypertensin, muscle weakness, hypokalaemia, abdominal pain and vomiting. They were not associated with long term sequalae or death.
Conclusion
In this study, we prove that regimens started with intravenous corticosteroids therapy are superior to oral regimen as they achieved higher levels of incremental increase in the hemoglobin levels from the baseline without increase of the incidence or increase the severity of the side effects. This is beneficial in cases of acute sever AIHA.
Keyword(s): Autoimmune hemolytic anemia (AIHA)