

Contributions
Abstract: EP522
Type: E-Poster Presentation
Session title: Aggressive Non-Hodgkin lymphoma - Clinical
Background
In aging society, the number of elderly patients with diffuse large B cell lymphoma (DLBCL) is increasing. The elderly patients cannot be managed in the same way as the young patients because of their various comorbidities and levels of frailty. However, the establishment of simple geriatric assessment tool to predict prognosis and management in treatment has rarely been reported in DLBCL.
Aims
The aim of this study was to verify the prognostic impact of the Geriatric 8 (G8) in elderly DLBCL patients, using a Cox hazards model with restricted cubic spline (RCS) model which is more suitable for reflecting the real-word practice.
Methods
To evaluate the usefulness of the G8, we conducted a retrospective, multicenter analysis of elderly DLBCL patients (≥65 years) who received standard therapy between 2007 and 2017 at three tertiary institutions in Japan. Patients treated with the standard regimen as first-line therapy were enrolled in this study. The exclusion criteria were transformed DLBCL, methotrexate-associated lymphoproliferative disorders, central nervous system involvement or undergoing treatment besides standard regimen. The standard regimen was defined as (R-) CHOP regimen (rituximab, cyclophosphamide, adriamycin [ADR], vincristine, and prednisolone) and (R-) THP-COP regimen (the same as CHOP including the doses, except tetrahydropyranyl adriamycin replaced ADR) in this study. The end point was the impact of the G8 on OS, which was defined as the interval from the date of the diagnosis to the date of all-cause death or the last follow-up visit. A multivariate Cox proportional hazards model was used to identify the predictors that were statistically associated with OS. Non-linear regression model with RCS was used to assess the presence of a non-linear relationship between the G8 score and OS. Diagnostic performance was assessed by receiver operating characteristic (ROC) analysis. The optimal G8 cutoff scores for OS were identified by ROC analysis using the Youden index. Survival curves for each group were estimated using the Kaplan-Meier method, and a comparison between risk groups was performed using the log-rank test.
Results
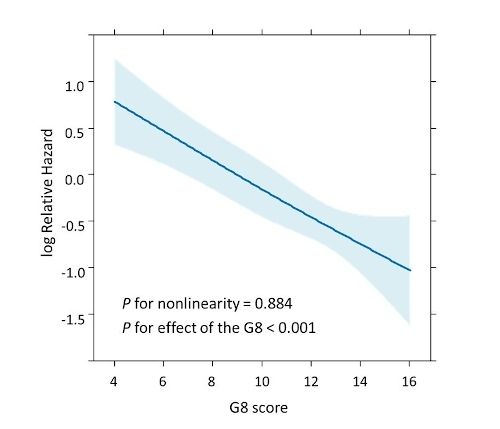
A total of 398 patients were included. With a median follow-up of 22.3 months (0-140.3), the estimated 2-year OS was 47.2%. A total of 196 patients (43.5%) died, including 127 (64.8%) of lymphoma and 10 (5.1%) of therapy-related toxicity. A multivariate Cox proportional hazards model demonstrated that the G8 was an IPI-independent prognostic predictor (HR 0.854, 95% CI 0.808-0.902, p<0.001). According to the multivariate RCS-Cox model, an obvious linear association was observed between G8 scores and mortality even though RCS model can represent in a nonlinear way (p for nonlinearity = 0.884, p for effect of the G8 <0.001). The lower the G8 score, the higher the risk of mortality. Especially, it was found that the mortality risk increases when the G8 score is below 9 to 10. The cutoff level of mortality, 9.5, in ROC analysis was considered robust, as it was consistent with the results of the Cox-RCS model. The Kaplan-Meier analysis showed that the patients with higher G8 had a significantly better prognosis than those with the lower G8 (log rank p<0.001).
Conclusion
Our research has revealed the G8 score was found to be an important prognostic predictor in elderly DLBCL patients, in that a lower G8 score proportionally exacerbated the prognosis.
Keyword(s): DLBCL, Elderly, Mortality
Abstract: EP522
Type: E-Poster Presentation
Session title: Aggressive Non-Hodgkin lymphoma - Clinical
Background
In aging society, the number of elderly patients with diffuse large B cell lymphoma (DLBCL) is increasing. The elderly patients cannot be managed in the same way as the young patients because of their various comorbidities and levels of frailty. However, the establishment of simple geriatric assessment tool to predict prognosis and management in treatment has rarely been reported in DLBCL.
Aims
The aim of this study was to verify the prognostic impact of the Geriatric 8 (G8) in elderly DLBCL patients, using a Cox hazards model with restricted cubic spline (RCS) model which is more suitable for reflecting the real-word practice.
Methods
To evaluate the usefulness of the G8, we conducted a retrospective, multicenter analysis of elderly DLBCL patients (≥65 years) who received standard therapy between 2007 and 2017 at three tertiary institutions in Japan. Patients treated with the standard regimen as first-line therapy were enrolled in this study. The exclusion criteria were transformed DLBCL, methotrexate-associated lymphoproliferative disorders, central nervous system involvement or undergoing treatment besides standard regimen. The standard regimen was defined as (R-) CHOP regimen (rituximab, cyclophosphamide, adriamycin [ADR], vincristine, and prednisolone) and (R-) THP-COP regimen (the same as CHOP including the doses, except tetrahydropyranyl adriamycin replaced ADR) in this study. The end point was the impact of the G8 on OS, which was defined as the interval from the date of the diagnosis to the date of all-cause death or the last follow-up visit. A multivariate Cox proportional hazards model was used to identify the predictors that were statistically associated with OS. Non-linear regression model with RCS was used to assess the presence of a non-linear relationship between the G8 score and OS. Diagnostic performance was assessed by receiver operating characteristic (ROC) analysis. The optimal G8 cutoff scores for OS were identified by ROC analysis using the Youden index. Survival curves for each group were estimated using the Kaplan-Meier method, and a comparison between risk groups was performed using the log-rank test.
Results
A total of 398 patients were included. With a median follow-up of 22.3 months (0-140.3), the estimated 2-year OS was 47.2%. A total of 196 patients (43.5%) died, including 127 (64.8%) of lymphoma and 10 (5.1%) of therapy-related toxicity. A multivariate Cox proportional hazards model demonstrated that the G8 was an IPI-independent prognostic predictor (HR 0.854, 95% CI 0.808-0.902, p<0.001). According to the multivariate RCS-Cox model, an obvious linear association was observed between G8 scores and mortality even though RCS model can represent in a nonlinear way (p for nonlinearity = 0.884, p for effect of the G8 <0.001). The lower the G8 score, the higher the risk of mortality. Especially, it was found that the mortality risk increases when the G8 score is below 9 to 10. The cutoff level of mortality, 9.5, in ROC analysis was considered robust, as it was consistent with the results of the Cox-RCS model. The Kaplan-Meier analysis showed that the patients with higher G8 had a significantly better prognosis than those with the lower G8 (log rank p<0.001).
Conclusion
Our research has revealed the G8 score was found to be an important prognostic predictor in elderly DLBCL patients, in that a lower G8 score proportionally exacerbated the prognosis.
Keyword(s): DLBCL, Elderly, Mortality