

Contributions
Abstract: EP473
Type: E-Poster Presentation
Session title: Acute myeloid leukemia - Clinical
Background
The achievement of a complete remission (CR) of acute myeloid leukemia (AML) after induction chemotherapy is an important factor for long-time survival. A good effect of the 1st induction cycle is a reduction of blast count to <5% in bone marrow on the day 15 or at the time of the blood count restitution. Otherwise, the patients receive the 2nd induction cycle, which can be based on the repeated 7+3 regimen as in the 1st induction cycle, or on a regimen with high-dose cytarabine. Resistant disease after the 2nd induction cycle has a poor prognosis. However, the prognosis of patients who achieved CR only after the 2nd induction cycle, compared to patients who achieved CR after the 1st induction cycle, is less clear.
Aims
First, to assess whether the relapse free survival (RFS) and the overall survival (OS) of patients who achieved CR only after the 2nd induction cycle differ from those who achieved CR after the 1st induction cycle. Second, to assess whether the type of regimen of the 2nd induction cycle (high-dose cytarabine regimens versus 7+3 regimen) correlates with CR rate, early death rate, RFS and OS of patients.
Methods
A retrospective analysis of real-world nationwide data from the database DATOOL-AML. Intensively treated adult patients with newly diagnosed AML (except AML M3) were included. The study period was 2007-2019.
Results
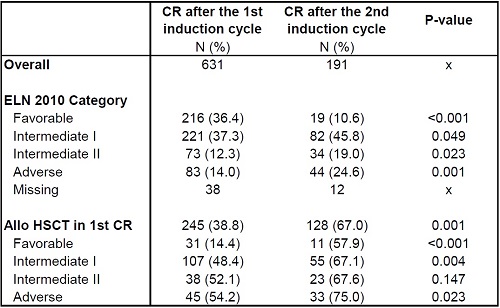
During the study period, 1010 patients (pts.) have initiated intensive induction chemotherapy; 631 (62.5%) pts. achieved CR after the 1st induction cycle (CR I group) and 191 (18.9%) pts. achieved CR only after the 2nd induction cycle (CR II group). The median age was 53 (18-74), the median follow-up was 24.7 months. There was a significantly higher proportion of intermediate I, intermediate II and adverse risk patients (ELN 2010 risk category) in the CRII group. On the contrary, the frequency of favorable risk patients in the CR II group was significantly lower, see Table 1. Allogeneic hematopoietic stem cell transplantation (HSCT) in the first CR was performed more frequently in CR II group and the difference was most evident in low and intermediate I risk categories, see Table 1. At 4 years, RFS of pts. in CR I group and in CR II group was 39.0% and 38.0%, respectively (p=0.179). At 4 years, OS of pts. in CR I group and CR II group was 52.6% and 46.2%, respectively (p=0.069). The high-dose cytarabine regimens administered during the 2nd induction cycle did not differ regarding the CR rate or early death rate in comparison to 7+3 regimen. CR rate after high-dose regimens versus 7+3 regimen was 62.4% and 69.8%, respectively (p=0.656), and early mortality rate was 6.6% and 4.7%, respectively (p=1.000). At 4 years, RFS of pts. treated by high-dose cytarabine regimens versus 7+3 regimen was 38.0% and 40.7% (p=0.449), and OS at 4 years was 43.3% and 68.8%, respectively (p=0.267).
Conclusion
We did not demonstrate any difference in RFS in patients who achieved CR after the 2nd induction cycle compared to patients who achieved CR after the 1st induction cycle. There was a trend in inferior OS of patients who achieved CR after the 2nd induction cycle, but it was not statistically relevant. The results might be explained by the significantly higher number of allogeneic HSCT performed in the first remission in patients who achieved CR after the 2nd induction cycle.
High-dose cytarabine reinduction regimens did not result in a substantial prolongation of RFS or OS compared to standard 7+3 regimen.
Keyword(s): AML, Induction chemotherapy
Abstract: EP473
Type: E-Poster Presentation
Session title: Acute myeloid leukemia - Clinical
Background
The achievement of a complete remission (CR) of acute myeloid leukemia (AML) after induction chemotherapy is an important factor for long-time survival. A good effect of the 1st induction cycle is a reduction of blast count to <5% in bone marrow on the day 15 or at the time of the blood count restitution. Otherwise, the patients receive the 2nd induction cycle, which can be based on the repeated 7+3 regimen as in the 1st induction cycle, or on a regimen with high-dose cytarabine. Resistant disease after the 2nd induction cycle has a poor prognosis. However, the prognosis of patients who achieved CR only after the 2nd induction cycle, compared to patients who achieved CR after the 1st induction cycle, is less clear.
Aims
First, to assess whether the relapse free survival (RFS) and the overall survival (OS) of patients who achieved CR only after the 2nd induction cycle differ from those who achieved CR after the 1st induction cycle. Second, to assess whether the type of regimen of the 2nd induction cycle (high-dose cytarabine regimens versus 7+3 regimen) correlates with CR rate, early death rate, RFS and OS of patients.
Methods
A retrospective analysis of real-world nationwide data from the database DATOOL-AML. Intensively treated adult patients with newly diagnosed AML (except AML M3) were included. The study period was 2007-2019.
Results
During the study period, 1010 patients (pts.) have initiated intensive induction chemotherapy; 631 (62.5%) pts. achieved CR after the 1st induction cycle (CR I group) and 191 (18.9%) pts. achieved CR only after the 2nd induction cycle (CR II group). The median age was 53 (18-74), the median follow-up was 24.7 months. There was a significantly higher proportion of intermediate I, intermediate II and adverse risk patients (ELN 2010 risk category) in the CRII group. On the contrary, the frequency of favorable risk patients in the CR II group was significantly lower, see Table 1. Allogeneic hematopoietic stem cell transplantation (HSCT) in the first CR was performed more frequently in CR II group and the difference was most evident in low and intermediate I risk categories, see Table 1. At 4 years, RFS of pts. in CR I group and in CR II group was 39.0% and 38.0%, respectively (p=0.179). At 4 years, OS of pts. in CR I group and CR II group was 52.6% and 46.2%, respectively (p=0.069). The high-dose cytarabine regimens administered during the 2nd induction cycle did not differ regarding the CR rate or early death rate in comparison to 7+3 regimen. CR rate after high-dose regimens versus 7+3 regimen was 62.4% and 69.8%, respectively (p=0.656), and early mortality rate was 6.6% and 4.7%, respectively (p=1.000). At 4 years, RFS of pts. treated by high-dose cytarabine regimens versus 7+3 regimen was 38.0% and 40.7% (p=0.449), and OS at 4 years was 43.3% and 68.8%, respectively (p=0.267).
Conclusion
We did not demonstrate any difference in RFS in patients who achieved CR after the 2nd induction cycle compared to patients who achieved CR after the 1st induction cycle. There was a trend in inferior OS of patients who achieved CR after the 2nd induction cycle, but it was not statistically relevant. The results might be explained by the significantly higher number of allogeneic HSCT performed in the first remission in patients who achieved CR after the 2nd induction cycle.
High-dose cytarabine reinduction regimens did not result in a substantial prolongation of RFS or OS compared to standard 7+3 regimen.
Keyword(s): AML, Induction chemotherapy