

Contributions
Abstract: EP1327
Type: E-Poster Presentation
Session title: Thrombosis and vascular biology - Biology & Translational Research
Background
During the follow-up of oral anticoagulation therapy (OAT) with vitamin K antagonists (VKA), the patient undergo invasive procedures. The decision wether to withdraw or maintain the OAT, as well as the needing or not to implement low molecular weight heparin (LMWH) as bridge therapy, will be determined by the patient's thrombotic risk (TR) and the haemorrhagic risk (HR) of the surgery.
Aims
To determine the incidence of thrombohemorrhagic complications in the periprocedural of the patient with OAT, limiting the use of LMWH to patients at high TR looking for decreasing bleeding events related to surgery.
Methods
Prospective, unicentric and observational study including 200 patients with OAT who had had surgery between December 2019 and February 2021, with a subsequent follow-up of 4 weeks. The periprocedural management of the OAT was carried out in the anticoagulation consultation according to the hospital protocol approved in the Thrombosis Committee, which classifies patients according to TR (High TR: Prosthetic heart valves, atrial fibrillation (AF) with CHA2DS2-VASc score 7-9, Severe rheumatic mitral valvulopathy, Venous Thromboembolism less tan 3 months ago and Severe thrombophilia, define as Leyden's factor V in homozygosis, 20210 prothrombin mutation, protein C, S or antithrombin III deficiency, múltiples deficiencys or Antiphospholipid Syndrome), and surgeries in three groups according to HR. Thus, the VKA is suspended 3 days before the intervention and resumed 24 hours after. The use of LMWH as bridge therapy (BT) is reserved for patients with high TR or suspected active cancer. It starts the moment OAT is suspended and it is reintroduced along with it 24 hours after surgery for 3 days (if there are no bleeding complications). The dose of LMWH is therapeutic (as patients requiring BT are high TR).
Given the coagulopathy inherent to COVID infection, no positive COVID patients were included.
Results
The median age of the population is 73 (range 33-93). The main reason for anticoagulation is AF (64.5%). Most patients are low TR and HR on the CHADs-VASc and HAS-BLED scales (76% and 64% respectively). 26.5% of the patients had personal history (PH) of thrombosis and 5.5% had PH of Hemorrhagic Diathesis.
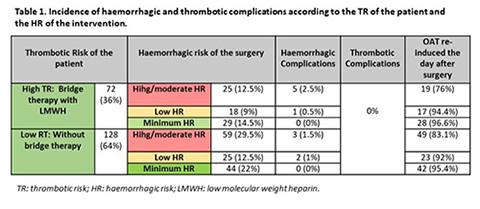
Table 1 shows the interventions performed and clinical events during the follow-up period. 10 post-surgical haemorrhagic events (5%) are described. Three of them (hemoperitoneum after cholecystectomy, hemoperitoneum after laparoscopic tubular gastrectomy, and haematoma of the anterior rectus abdominis muscle with secondary anemization after ventral hernia repair) required hospitalisation for management, all of which were solved with conservative treatment. The other 7 were mild events that were handled outpatiently. In addition, intra-procedure bleeding during bronchoscopy is described in patient with BT, that was controlled on the spot with amchafibrin and adrenaline. No thrombotic events were recorded. Generally, OAT was re-induced the day after surgery in patients undergoing minimal and low HR interventions, being the percentage somewhat lower in patients undergoing high HR interventions, both in high or low TR patients.
Conclusion
Standardization by means of a periprocedural management protocol of the OAT that adjusts BT with LMWH according to the risk factors of each patient, results in a reduction of the incidence of haemorrhagic complications without secondary increase of thromboembolic events. This study demonstrates the importance of centralizing unified periprocedural management using an established protocol.
Keyword(s): Bleeding, Heparin, Surgery, Thrombosis
Abstract: EP1327
Type: E-Poster Presentation
Session title: Thrombosis and vascular biology - Biology & Translational Research
Background
During the follow-up of oral anticoagulation therapy (OAT) with vitamin K antagonists (VKA), the patient undergo invasive procedures. The decision wether to withdraw or maintain the OAT, as well as the needing or not to implement low molecular weight heparin (LMWH) as bridge therapy, will be determined by the patient's thrombotic risk (TR) and the haemorrhagic risk (HR) of the surgery.
Aims
To determine the incidence of thrombohemorrhagic complications in the periprocedural of the patient with OAT, limiting the use of LMWH to patients at high TR looking for decreasing bleeding events related to surgery.
Methods
Prospective, unicentric and observational study including 200 patients with OAT who had had surgery between December 2019 and February 2021, with a subsequent follow-up of 4 weeks. The periprocedural management of the OAT was carried out in the anticoagulation consultation according to the hospital protocol approved in the Thrombosis Committee, which classifies patients according to TR (High TR: Prosthetic heart valves, atrial fibrillation (AF) with CHA2DS2-VASc score 7-9, Severe rheumatic mitral valvulopathy, Venous Thromboembolism less tan 3 months ago and Severe thrombophilia, define as Leyden's factor V in homozygosis, 20210 prothrombin mutation, protein C, S or antithrombin III deficiency, múltiples deficiencys or Antiphospholipid Syndrome), and surgeries in three groups according to HR. Thus, the VKA is suspended 3 days before the intervention and resumed 24 hours after. The use of LMWH as bridge therapy (BT) is reserved for patients with high TR or suspected active cancer. It starts the moment OAT is suspended and it is reintroduced along with it 24 hours after surgery for 3 days (if there are no bleeding complications). The dose of LMWH is therapeutic (as patients requiring BT are high TR).
Given the coagulopathy inherent to COVID infection, no positive COVID patients were included.
Results
The median age of the population is 73 (range 33-93). The main reason for anticoagulation is AF (64.5%). Most patients are low TR and HR on the CHADs-VASc and HAS-BLED scales (76% and 64% respectively). 26.5% of the patients had personal history (PH) of thrombosis and 5.5% had PH of Hemorrhagic Diathesis.
Table 1 shows the interventions performed and clinical events during the follow-up period. 10 post-surgical haemorrhagic events (5%) are described. Three of them (hemoperitoneum after cholecystectomy, hemoperitoneum after laparoscopic tubular gastrectomy, and haematoma of the anterior rectus abdominis muscle with secondary anemization after ventral hernia repair) required hospitalisation for management, all of which were solved with conservative treatment. The other 7 were mild events that were handled outpatiently. In addition, intra-procedure bleeding during bronchoscopy is described in patient with BT, that was controlled on the spot with amchafibrin and adrenaline. No thrombotic events were recorded. Generally, OAT was re-induced the day after surgery in patients undergoing minimal and low HR interventions, being the percentage somewhat lower in patients undergoing high HR interventions, both in high or low TR patients.
Conclusion
Standardization by means of a periprocedural management protocol of the OAT that adjusts BT with LMWH according to the risk factors of each patient, results in a reduction of the incidence of haemorrhagic complications without secondary increase of thromboembolic events. This study demonstrates the importance of centralizing unified periprocedural management using an established protocol.
Keyword(s): Bleeding, Heparin, Surgery, Thrombosis