

Contributions
Abstract: EP1311
Type: E-Poster Presentation
Session title: Thalassemias
Background
Current therapeutic modalities has rendered thalassemia a chronic disease. With patients’ advanced age, previously unknown complications are observed with increasing frequency. Among them, liver disease and hepatocellular carcinoma(HCC) are on the rise. Viral hepatitis, mainly hepatitis C, and chronic iron overload are the main causes of liver disease, presenting as significant fibrosis, cirrhosis and/or HCC. Direct histological examination of hepatic tissue obtained by biopsy, remains highly sensitive and specific for the diagnosis of liver disease, but its predictive value is not established.
Aims
To evaluate the predictive value of histological findings of liver biopsy in the long-term liver-related morbidity and mortality in patients with β-thalassemia.
Methods
A retrospective analysis was performed in a group of Transfusion-Dependent (TDT) or Non-Transfusion-Dependent (NTDT) β-Thalassemia patients, who had undergone liver biopsy from 1992 to 2005, and were followed till 31/12/2020 in a single institution. Severe hepatic events were defined as either liver cirrhosis, HCC or death due to liver disease.Kaplan-Meier estimator was used to estimate disease-free survival (DFS). Cox proportional hazards model or Peto&Peto modification of the Gehan-Wilcoxon test were used to investigate risk factors. Time-To-Event (TTE) was performed from the date of: (1) birth or (2) biopsy, to the date of the liver event or of last follow up for censored records. The association of siderosis burden with ferritin was assessed through the Mann-Whitney U test. Statistical analysis was conducted using RStudio v. 3.6.3.
Results
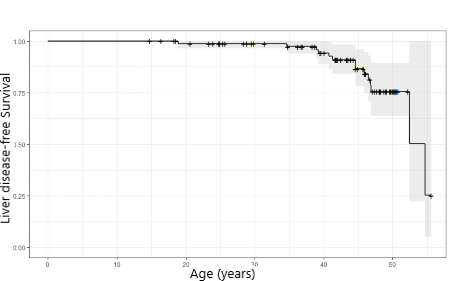
In total, 87 patients (54 males, 79 TDT) had undergone liver biopsy at the age of 21.8±6.1 years and were monitored for 19.4 (IQR; 14.3-27.9) years. Forty-eight patients (55.2%) had viral hepatitis C. Histology evaluation showed low siderosis (grade:0-2 in a scale of 0-4) in 34 (39.1%) and high siderosis (grade: 3-4) in 50 (57.5%) patients, while it was not reported in 3 (3.4%). Mild fibrosis (grade: 0-2 in a scale of 0-6, as per Ishak classification) was observed in 22 (25.3%) patients, advanced fibrosis (grade 3-6) in 62 (71.3%), while in 3 patients was not recorded. We identified 14 (16.1%) events (all in TDT patients);7 developed HCC, 4 liver cirrhosis and 3 died from other liver-related causes. At 50 years of age DFS was 75% (figure 1), while 25% of patients developed liver disease in 24.4 years after the date of biopsy.High siderosis carries a greater risk for developing liver disease compared to group with low siderosis, Hazard Ratio (HR) 3.00 (95% CI:1.01-8.95, p=0.05), adjusted for age (aHR) 2.9 (95% CI: 0.90 – 9.01, p=0.07). An increase of 50 μg/L in ferritin level at time of biopsy is associated with an increased risk of developing liver disease (aHR 1.02, 95% CI:1.00-1.03, p=0.03). A statistically significant correlation was observed between high serum ferritin levels and high siderosis at the date of biopsy (1712(IQR;1000-2985) vs 3715(IQR;1721-5197.5),p=0.0003). No statistically significant correlation in the development of liver disease was observed between gender, HCV and degree of fibrosis at time of biopsy, p=0.2, p=0.3 and p=0.2, respectively.
Conclusion
The occurrence of liver-disease is increasing after the 4th decade of life. Serum ferritin and liver siderosis at the time of biopsy was found to be statistically significant risk factors for the progression of the disease. Degree of liver fibrosis does not seem to be related to progression, which may be due to stabilization and/or reversal of fibrosis achieved with current chelation therapy.
Keyword(s): Liver biopsy, Liver disease, Thalassemia
Abstract: EP1311
Type: E-Poster Presentation
Session title: Thalassemias
Background
Current therapeutic modalities has rendered thalassemia a chronic disease. With patients’ advanced age, previously unknown complications are observed with increasing frequency. Among them, liver disease and hepatocellular carcinoma(HCC) are on the rise. Viral hepatitis, mainly hepatitis C, and chronic iron overload are the main causes of liver disease, presenting as significant fibrosis, cirrhosis and/or HCC. Direct histological examination of hepatic tissue obtained by biopsy, remains highly sensitive and specific for the diagnosis of liver disease, but its predictive value is not established.
Aims
To evaluate the predictive value of histological findings of liver biopsy in the long-term liver-related morbidity and mortality in patients with β-thalassemia.
Methods
A retrospective analysis was performed in a group of Transfusion-Dependent (TDT) or Non-Transfusion-Dependent (NTDT) β-Thalassemia patients, who had undergone liver biopsy from 1992 to 2005, and were followed till 31/12/2020 in a single institution. Severe hepatic events were defined as either liver cirrhosis, HCC or death due to liver disease.Kaplan-Meier estimator was used to estimate disease-free survival (DFS). Cox proportional hazards model or Peto&Peto modification of the Gehan-Wilcoxon test were used to investigate risk factors. Time-To-Event (TTE) was performed from the date of: (1) birth or (2) biopsy, to the date of the liver event or of last follow up for censored records. The association of siderosis burden with ferritin was assessed through the Mann-Whitney U test. Statistical analysis was conducted using RStudio v. 3.6.3.
Results
In total, 87 patients (54 males, 79 TDT) had undergone liver biopsy at the age of 21.8±6.1 years and were monitored for 19.4 (IQR; 14.3-27.9) years. Forty-eight patients (55.2%) had viral hepatitis C. Histology evaluation showed low siderosis (grade:0-2 in a scale of 0-4) in 34 (39.1%) and high siderosis (grade: 3-4) in 50 (57.5%) patients, while it was not reported in 3 (3.4%). Mild fibrosis (grade: 0-2 in a scale of 0-6, as per Ishak classification) was observed in 22 (25.3%) patients, advanced fibrosis (grade 3-6) in 62 (71.3%), while in 3 patients was not recorded. We identified 14 (16.1%) events (all in TDT patients);7 developed HCC, 4 liver cirrhosis and 3 died from other liver-related causes. At 50 years of age DFS was 75% (figure 1), while 25% of patients developed liver disease in 24.4 years after the date of biopsy.High siderosis carries a greater risk for developing liver disease compared to group with low siderosis, Hazard Ratio (HR) 3.00 (95% CI:1.01-8.95, p=0.05), adjusted for age (aHR) 2.9 (95% CI: 0.90 – 9.01, p=0.07). An increase of 50 μg/L in ferritin level at time of biopsy is associated with an increased risk of developing liver disease (aHR 1.02, 95% CI:1.00-1.03, p=0.03). A statistically significant correlation was observed between high serum ferritin levels and high siderosis at the date of biopsy (1712(IQR;1000-2985) vs 3715(IQR;1721-5197.5),p=0.0003). No statistically significant correlation in the development of liver disease was observed between gender, HCV and degree of fibrosis at time of biopsy, p=0.2, p=0.3 and p=0.2, respectively.
Conclusion
The occurrence of liver-disease is increasing after the 4th decade of life. Serum ferritin and liver siderosis at the time of biopsy was found to be statistically significant risk factors for the progression of the disease. Degree of liver fibrosis does not seem to be related to progression, which may be due to stabilization and/or reversal of fibrosis achieved with current chelation therapy.
Keyword(s): Liver biopsy, Liver disease, Thalassemia