

Contributions
Abstract: EP1292
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Cutaneous T-cell lymphomas (CTCL) are a heterogenous group of T-cell non-Hodgkin lymphomas with a variable prognosis. Patients with mycosis fungoides (MF) can have indolent disease, however transformed MF and Sezary Syndrome (SS) have an aggressive clinical course. CTCL are incurable with systemic chemotherapy but can achieve durable remissions with allogeneic stem cell transplantation (allo-SCT) and an SCT program was initiated for this group of poor prognosis patients in 2004 at a National allo-SCT Centre.
Aims
To review outcomes of consecutive patients with CTCL undergoing allo-SCT.
Methods
Patient demographics, disease characteristics, and outcome data were collected on consecutive CTCL patients transplanted from 2010 - 2020 at the Republic of Ireland (ROI) National allo-SCT Unit using 3 conditioning regimens; transformed MF <45 years received Cy-TBI, patients willing to travel outside ROI for Total Skin Electron Beam therapy (TSEBT) received TSEBT, total nodal irradiation, Anti-Thymocyte Globulin (ATG) and mycophenolate mofetil (Stanford) conditioning and the remaining patients received standard reduced intensity conditioning (RIC) with Flu-Mel-ATG. Graft versus host disease (GVHD) prophylaxis with ciclosporin (+/- methotrexate) was used.
Results
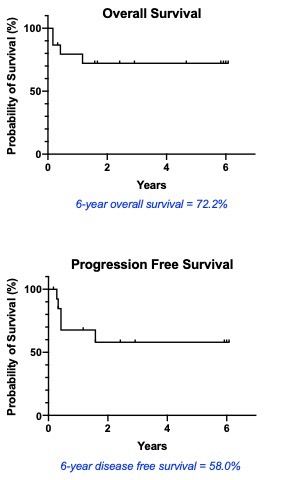
Fifteen patients (10 male, 5 female) underwent allo-SCT with a median age at transplant of 49 years (range 21-64). Eight patients had SS, while 4 of 7 patients with MF had transformed disease. All four transformed MF patients [one of whom received pre-transplant brentuximab vedotin (BV)] expressed CD30. Ten patients had Stage IV disease (revised ISCL/EORTC criteria) and 7 patients had a raised LDH at referral for allo-SCT. Eleven patients (7 MF, 4 SS) received systemic chemotherapy (range 1-3 lines) pre allo-SCT; remission status pre-transplant consisted of 2 complete remissions, 10 partial remissions and 3 stable disease. Five MF patients recieved Cy/TBI conditioning, 4 SS patients received Stanford, and 6 patients (4 SS, 2 MF) received Flu-Mel-ATG conditioning. Neutrophil and platelet engraftment occurred at a median of 15 and 14.5 days respectively. Acute GVHD occurred in 13 patients, all of whom had grade 3 skin GVHD, while 5 patients had concomitant gut GVHD (grade 1-3). Early treatment-related mortality (TRM) occurred in 2 patients; one from CMV pneumonitis following Stanford conditioning and one from pneumonia following Cy-TBI. One patient progressed following Cy-TBI at 102 days and died 5 months post allo-SCT, one patient died 14 months post allo-SCT from viral pneumonitis. There were 4 overt relapses at a range of 4-19 months; 3 received donor lymphocyte infusion (DLI) and 1 had immunosuppression weaned; all 4 are in CR with a median follow up of 42 months. OS and PFS at 6 years were 72.2% and 58.0% respectively.
Conclusion
OS and PFS in this allo-SCT cohort of 15 CTCL patients was 72.2% and 58% with 4 patients achieving meaningful remissions with DLI despite post allo-SCT relapses. SS patients referred early in the disease course, had a good outcome with one post allo-SCT relapse. There were no relapses in SS patients receiving Stanford conditioning. MF patients did less well, but were referred for allo-SCT with advanced/transformed disease and may benefit (1) from earlier transplant referral and (2) from BV treatment if CD30 positive pre allo-SCT. Allo-SCT is an appropriate treatment for advanced CTCL, however improving referral timelines and conditioning in MF and reducing the incidence of skin GVHD remain challenges.
Keyword(s): Allogeneic stem cell transplant, Cutaneous T-cell lymphoma, Mycosis fungoides
Abstract: EP1292
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Cutaneous T-cell lymphomas (CTCL) are a heterogenous group of T-cell non-Hodgkin lymphomas with a variable prognosis. Patients with mycosis fungoides (MF) can have indolent disease, however transformed MF and Sezary Syndrome (SS) have an aggressive clinical course. CTCL are incurable with systemic chemotherapy but can achieve durable remissions with allogeneic stem cell transplantation (allo-SCT) and an SCT program was initiated for this group of poor prognosis patients in 2004 at a National allo-SCT Centre.
Aims
To review outcomes of consecutive patients with CTCL undergoing allo-SCT.
Methods
Patient demographics, disease characteristics, and outcome data were collected on consecutive CTCL patients transplanted from 2010 - 2020 at the Republic of Ireland (ROI) National allo-SCT Unit using 3 conditioning regimens; transformed MF <45 years received Cy-TBI, patients willing to travel outside ROI for Total Skin Electron Beam therapy (TSEBT) received TSEBT, total nodal irradiation, Anti-Thymocyte Globulin (ATG) and mycophenolate mofetil (Stanford) conditioning and the remaining patients received standard reduced intensity conditioning (RIC) with Flu-Mel-ATG. Graft versus host disease (GVHD) prophylaxis with ciclosporin (+/- methotrexate) was used.
Results
Fifteen patients (10 male, 5 female) underwent allo-SCT with a median age at transplant of 49 years (range 21-64). Eight patients had SS, while 4 of 7 patients with MF had transformed disease. All four transformed MF patients [one of whom received pre-transplant brentuximab vedotin (BV)] expressed CD30. Ten patients had Stage IV disease (revised ISCL/EORTC criteria) and 7 patients had a raised LDH at referral for allo-SCT. Eleven patients (7 MF, 4 SS) received systemic chemotherapy (range 1-3 lines) pre allo-SCT; remission status pre-transplant consisted of 2 complete remissions, 10 partial remissions and 3 stable disease. Five MF patients recieved Cy/TBI conditioning, 4 SS patients received Stanford, and 6 patients (4 SS, 2 MF) received Flu-Mel-ATG conditioning. Neutrophil and platelet engraftment occurred at a median of 15 and 14.5 days respectively. Acute GVHD occurred in 13 patients, all of whom had grade 3 skin GVHD, while 5 patients had concomitant gut GVHD (grade 1-3). Early treatment-related mortality (TRM) occurred in 2 patients; one from CMV pneumonitis following Stanford conditioning and one from pneumonia following Cy-TBI. One patient progressed following Cy-TBI at 102 days and died 5 months post allo-SCT, one patient died 14 months post allo-SCT from viral pneumonitis. There were 4 overt relapses at a range of 4-19 months; 3 received donor lymphocyte infusion (DLI) and 1 had immunosuppression weaned; all 4 are in CR with a median follow up of 42 months. OS and PFS at 6 years were 72.2% and 58.0% respectively.
Conclusion
OS and PFS in this allo-SCT cohort of 15 CTCL patients was 72.2% and 58% with 4 patients achieving meaningful remissions with DLI despite post allo-SCT relapses. SS patients referred early in the disease course, had a good outcome with one post allo-SCT relapse. There were no relapses in SS patients receiving Stanford conditioning. MF patients did less well, but were referred for allo-SCT with advanced/transformed disease and may benefit (1) from earlier transplant referral and (2) from BV treatment if CD30 positive pre allo-SCT. Allo-SCT is an appropriate treatment for advanced CTCL, however improving referral timelines and conditioning in MF and reducing the incidence of skin GVHD remain challenges.
Keyword(s): Allogeneic stem cell transplant, Cutaneous T-cell lymphoma, Mycosis fungoides