

Contributions
Abstract: EP1284
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Allogeneic hematopoietic stem cell transplantation is the only curative therapy for myelofibrosis but is often complicated by graft failure and high rates of relapse. The optimal conditioning regimen has not been well determined. In order to improve outcomes, our center has transplanted patients with myelofibrosis with a conditioning regimen consisting of fludarabine, treosulfan and ATG, a regiment that was previously used for second transplant after primary graft failure.
Aims
The aim of this study was to analyze the outcomes of allogeneic hematopoietic stem cell transplantation after conditioning with fludarabine, treosulfan and ATG, in terms of engraftment, relapse, non-relapse mortality, relapse-free-graft-versus-host-free survival and overall survival.
Methods
We analyzed outcomes in patients with myelofibrosis (n = 21) after allogeneic stem cell transplantation preceded by fludarabine, treosulfan and ATG (anti-thymocyte thymoglobulin) conditioning, in a retrospective single center cohort study.
Results
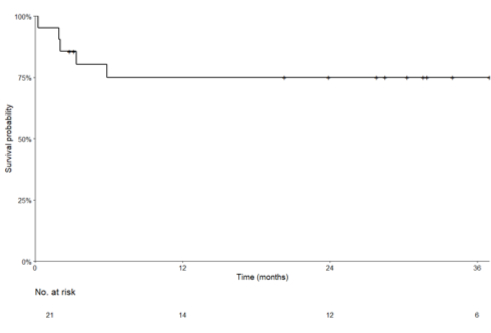
Patients were transplanted with stem cells from siblings (n = 4), HLA 10/10 matched unrelated donors (n=15) or HLA 9/10 mismatched unrelated donors (n = 2) between the years 2014 and 2020. The median follow-up was 2.3 years for all patients (range 0.3 - 6,1).
Median time of engraftment was 17 days and all patients were engrafted within 32 days. Mean donor chimerism at day 30-35 was 99% (T-cell and mononuclear cells). Incidence of grade III-IV acute graft versus host disease (GVHD) was 25%, of whom 60% of patients achieved complete remission with prednisolone, tacrolimus and/or ruxolitinib. Incidence of chronic GVHD was 39%, of which 71% classified as NIH stage mild. We observed high rates of EBV reactivation (86%, all responsive to rituximab) and CMV reactivation (43%), the latter often followed by development of acute GVHD. Non-relapse mortality at 1 year was 19%. The 2-year progression-free survival was 92%, the 2-year relapse-free-graft-versus-host-disease-free survival was 38%. 1 year overall survival was 76%.
Conclusion
Our results indicate that conditioning with fludarabine, treosulfan and prior to allogeneic hematopoietic stem cell transplantation for myelofibrosis results in excellent engraftment and low rates of relapse and non-relapse mortality, leading to a high overall survival.
Keyword(s): Allogeneic hematopoietic stem cell transplant, Conditioning, Myelofibrosis
Abstract: EP1284
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Allogeneic hematopoietic stem cell transplantation is the only curative therapy for myelofibrosis but is often complicated by graft failure and high rates of relapse. The optimal conditioning regimen has not been well determined. In order to improve outcomes, our center has transplanted patients with myelofibrosis with a conditioning regimen consisting of fludarabine, treosulfan and ATG, a regiment that was previously used for second transplant after primary graft failure.
Aims
The aim of this study was to analyze the outcomes of allogeneic hematopoietic stem cell transplantation after conditioning with fludarabine, treosulfan and ATG, in terms of engraftment, relapse, non-relapse mortality, relapse-free-graft-versus-host-free survival and overall survival.
Methods
We analyzed outcomes in patients with myelofibrosis (n = 21) after allogeneic stem cell transplantation preceded by fludarabine, treosulfan and ATG (anti-thymocyte thymoglobulin) conditioning, in a retrospective single center cohort study.
Results
Patients were transplanted with stem cells from siblings (n = 4), HLA 10/10 matched unrelated donors (n=15) or HLA 9/10 mismatched unrelated donors (n = 2) between the years 2014 and 2020. The median follow-up was 2.3 years for all patients (range 0.3 - 6,1).
Median time of engraftment was 17 days and all patients were engrafted within 32 days. Mean donor chimerism at day 30-35 was 99% (T-cell and mononuclear cells). Incidence of grade III-IV acute graft versus host disease (GVHD) was 25%, of whom 60% of patients achieved complete remission with prednisolone, tacrolimus and/or ruxolitinib. Incidence of chronic GVHD was 39%, of which 71% classified as NIH stage mild. We observed high rates of EBV reactivation (86%, all responsive to rituximab) and CMV reactivation (43%), the latter often followed by development of acute GVHD. Non-relapse mortality at 1 year was 19%. The 2-year progression-free survival was 92%, the 2-year relapse-free-graft-versus-host-disease-free survival was 38%. 1 year overall survival was 76%.
Conclusion
Our results indicate that conditioning with fludarabine, treosulfan and prior to allogeneic hematopoietic stem cell transplantation for myelofibrosis results in excellent engraftment and low rates of relapse and non-relapse mortality, leading to a high overall survival.
Keyword(s): Allogeneic hematopoietic stem cell transplant, Conditioning, Myelofibrosis