

Contributions
Abstract: EP1247
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Allogeneic hematopoietic stem cell transplant (HSCT) is a standard therapy for patients with acute myeloid leukemia (AML), when the risk for relapse overweighs projected transplant related morbidity and mortality. Disease relapse remains the most common reason for transplant failure and patient death, and treatment of relapse remains extremely challenging. Reducing the risk of post-transplant relapse without unwanted toxicity by means of post-transplant maintenance therapy has recently been studied in several prospective studies.
Aims
We aimed to evaluate the efficacy and safety of maintenance therapy for AML after allogeneic HSCT.
Methods
Systematic review and meta-analysis of randomized controlled trials which compared maintenance therapy with observation or placebo in AML patients after allogeneic HSCT. The Cochrane Library, Pubmed, conference proceedings and references were searched until February 2021. Two reviewers appraised the quality of trials and extracted data. Primary outcome was overall survival (OS). Secondary outcomes included relapse free survival (RFS), relapse rate and safety (including adverse events and GVHD).
Results
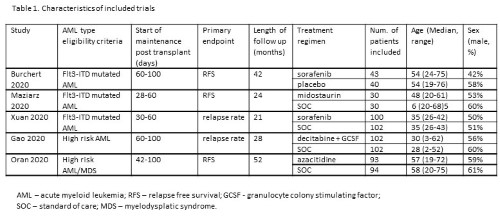
Our search yielded five trials conducted between the years 2009 and 2018, including 736 patients, all published in peer-reviewed journals. Maintenance therapy was comprised of tyrosine kinase inhibitors (TKI): sorafenib - 2 studies; midostaurin - 1 study, and hypomethylating agents (HMAs): decitabine and azacytidine - one study each. Characteristics of included trials are presented in Table 1. Data from four trials were available for analysis of OS. Maintenance after allogeneic HSCT was associated with an improved OS, HR=0.61 (95% CI 0.47-0.80, I2=2%, 547 patients). Subgroup analyses by type of maintenance therapy also revealed advantage in OS with either TKI or HMA maintenance [HR=0.50 (95% CI 0.33-0.77, 3 trials, 345 patients) and HR=0.69 (95% CI 0.49-0.98, 2 trials, 391 patients), respectively]. Data from five trials were available for RFS analysis and showed improved RFS in the maintenance group compared with the control arm HR=0.51 [95% CI 0.40 - 0.66]. Relapse rate was significantly decreased in the maintenance arm compared to the control arm, RR=0.41 (95% CI 0.20-0.88, 4 trials, 668 patients).
Regarding safety, three trials reported grade 3 or 4 adverse events. The risk of any grade 3 or 4 adverse events did not increase with the addition of maintenance after allogeneic HSCT, RR=1.0 (95% CI 0.83-1.20, 464 patients). There was no difference between the maintenance and control arms in the rate of all infections or grade 3 or 4 infections [(RR=0.98 (95% CI 0.83-1.16, I2=0%, 3 trials, 585 patients) and (RR=0.96 (95% CI 0.68-1.36, 3 trials, 464 patients), respectively]. There was no difference between the two arms in grade 3 or 4 thrombocytopenia or in grade 3 or 4 neutropenia. No difference was noted between the two arms regarding grade 2-4 acute GVHD, mild-moderate chronic GVHD or severe chronic GVHD.
Conclusion
Our meta-analysis shows that post-transplant maintenance therapy in AML patients is effective in decreasing relapse rate and improving RFS and OS, with a satisfactory safety profile.
Keyword(s): Acute myeloid leukemia, Hematopoietic cell transplantation, Maintenance
Abstract: EP1247
Type: E-Poster Presentation
Session title: Stem cell transplantation - Clinical
Background
Allogeneic hematopoietic stem cell transplant (HSCT) is a standard therapy for patients with acute myeloid leukemia (AML), when the risk for relapse overweighs projected transplant related morbidity and mortality. Disease relapse remains the most common reason for transplant failure and patient death, and treatment of relapse remains extremely challenging. Reducing the risk of post-transplant relapse without unwanted toxicity by means of post-transplant maintenance therapy has recently been studied in several prospective studies.
Aims
We aimed to evaluate the efficacy and safety of maintenance therapy for AML after allogeneic HSCT.
Methods
Systematic review and meta-analysis of randomized controlled trials which compared maintenance therapy with observation or placebo in AML patients after allogeneic HSCT. The Cochrane Library, Pubmed, conference proceedings and references were searched until February 2021. Two reviewers appraised the quality of trials and extracted data. Primary outcome was overall survival (OS). Secondary outcomes included relapse free survival (RFS), relapse rate and safety (including adverse events and GVHD).
Results
Our search yielded five trials conducted between the years 2009 and 2018, including 736 patients, all published in peer-reviewed journals. Maintenance therapy was comprised of tyrosine kinase inhibitors (TKI): sorafenib - 2 studies; midostaurin - 1 study, and hypomethylating agents (HMAs): decitabine and azacytidine - one study each. Characteristics of included trials are presented in Table 1. Data from four trials were available for analysis of OS. Maintenance after allogeneic HSCT was associated with an improved OS, HR=0.61 (95% CI 0.47-0.80, I2=2%, 547 patients). Subgroup analyses by type of maintenance therapy also revealed advantage in OS with either TKI or HMA maintenance [HR=0.50 (95% CI 0.33-0.77, 3 trials, 345 patients) and HR=0.69 (95% CI 0.49-0.98, 2 trials, 391 patients), respectively]. Data from five trials were available for RFS analysis and showed improved RFS in the maintenance group compared with the control arm HR=0.51 [95% CI 0.40 - 0.66]. Relapse rate was significantly decreased in the maintenance arm compared to the control arm, RR=0.41 (95% CI 0.20-0.88, 4 trials, 668 patients).
Regarding safety, three trials reported grade 3 or 4 adverse events. The risk of any grade 3 or 4 adverse events did not increase with the addition of maintenance after allogeneic HSCT, RR=1.0 (95% CI 0.83-1.20, 464 patients). There was no difference between the maintenance and control arms in the rate of all infections or grade 3 or 4 infections [(RR=0.98 (95% CI 0.83-1.16, I2=0%, 3 trials, 585 patients) and (RR=0.96 (95% CI 0.68-1.36, 3 trials, 464 patients), respectively]. There was no difference between the two arms in grade 3 or 4 thrombocytopenia or in grade 3 or 4 neutropenia. No difference was noted between the two arms regarding grade 2-4 acute GVHD, mild-moderate chronic GVHD or severe chronic GVHD.
Conclusion
Our meta-analysis shows that post-transplant maintenance therapy in AML patients is effective in decreasing relapse rate and improving RFS and OS, with a satisfactory safety profile.
Keyword(s): Acute myeloid leukemia, Hematopoietic cell transplantation, Maintenance