

Contributions
Abstract: EP1166
Type: E-Poster Presentation
Session title: Quality of life, palliative care, ethics and health economics
Background
AL is caused by the amyloid deposition of a misfolded protein responsible for organ damage. In men, ED can be an early disease related feature, but the real incidence and pathogenesis is not well established. ED can be psychogenic or organic.
Aims
Our aim is to investigate the incidence and evaluate the presence and possible causes of ED in male patients with AL.
Methods
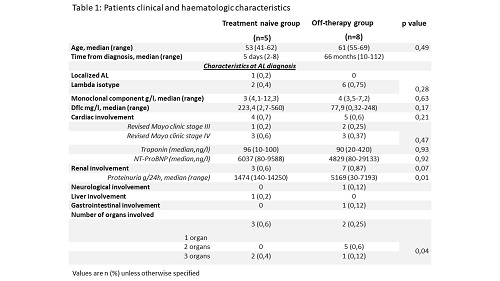
All male adult patients with a confirmed diagnosis of AL attending the Haematology Department of Federico II University were enrolled in the study, from July to November 2020. Patients older than 70 years and/or with ECOG ≥ 2 were excluded. All patients underwent a diagnostic work up, comprehensive of hematologic and andrological assessments. Andrological assessment, performed by G.F and P.R, consisted in physical examination, power doppler ultra-sound (PDUS) evaluation and a structured questionnaire concerning sexual activity [International Index of Erectile Function (IIEF-15)]. Mayo clinic staging assessment was reported for all patients at diagnosis and enrolment (Table).
Results
A total of 13 patients were included (Table): five patients were enrolled at AL diagnosis (“treatment naïve”) while eight patients were in follow-up after Bortezomib-based treatment (“Off-therapy”). In the latter group, hematologic complete response and Very Good Partial Response were observed in 5/8 and 3/8 patients, respectively (median 38 and 57 months, respectively); complete organ response was recorded in all patients. Assessments of hormonal dosages resulted within the reference limit for all patients and nobody resulted suffering from pathological depression according to our psychologist consultant (S.A). ED prevalence was 92.3% (12/13): 9 subjects with severe ED, 1 with moderate ED, and 2 with mild ED (the patient with localized AL was the only one not suffering from ED). The flowmetric indices showed a reduction of peak systolic value (PSV) in 76.9% of patients and a pathological acceleration (Acc) in 4/13. The population was analyzed based on both andrological and haematologic characteristics. Patients with pathological Acc showed a higher age (p=0.05) and worse scores at IIEF-TOT (p=0.006), at Desire Function (p=0.011), at Overall Satisfaction (p=0.034); patients with severe ED showed a higher age (p value = 0,003) and a pathological left Acc value (p value= 0,04); patients with mild ED and patient with normal erectile function (localized AL) showed normal right PSV (P value = 0,004) and normal left PSV (p value= 0,006) in comparison with patients with moderate and severe ED. Overall, no statistical difference was found for the two groups of patients: ED prevalence and ED stage was homogenous as the flowmetric characteristics. In the “off-therapy” group no differences were found according to hematologic response.
Conclusion
In our study a strong association between arterial inflow deficit, penile hemodynamic alteration, and ED was outlined. Having ruled out all possible causes for secondary ED, an arteriogenic cause, sustained by a possible cardiotoxic effect of extracellular light chain, was disclosed by the presence of early endothelial dysfunction in systemic AL patients independently of AL treatment received, time from AL diagnosis and organ involvement (the patient with localized AL was the only one not suffering from ED). A possible indication our study may provide is that any patient seeking medical advice for unexplained ED (common secondary ED causes ruled out) should undergo AL screening with QPE and FLC assay.
Keyword(s): Amyloidosis, Chemotherapy, Quality of life
Abstract: EP1166
Type: E-Poster Presentation
Session title: Quality of life, palliative care, ethics and health economics
Background
AL is caused by the amyloid deposition of a misfolded protein responsible for organ damage. In men, ED can be an early disease related feature, but the real incidence and pathogenesis is not well established. ED can be psychogenic or organic.
Aims
Our aim is to investigate the incidence and evaluate the presence and possible causes of ED in male patients with AL.
Methods
All male adult patients with a confirmed diagnosis of AL attending the Haematology Department of Federico II University were enrolled in the study, from July to November 2020. Patients older than 70 years and/or with ECOG ≥ 2 were excluded. All patients underwent a diagnostic work up, comprehensive of hematologic and andrological assessments. Andrological assessment, performed by G.F and P.R, consisted in physical examination, power doppler ultra-sound (PDUS) evaluation and a structured questionnaire concerning sexual activity [International Index of Erectile Function (IIEF-15)]. Mayo clinic staging assessment was reported for all patients at diagnosis and enrolment (Table).
Results
A total of 13 patients were included (Table): five patients were enrolled at AL diagnosis (“treatment naïve”) while eight patients were in follow-up after Bortezomib-based treatment (“Off-therapy”). In the latter group, hematologic complete response and Very Good Partial Response were observed in 5/8 and 3/8 patients, respectively (median 38 and 57 months, respectively); complete organ response was recorded in all patients. Assessments of hormonal dosages resulted within the reference limit for all patients and nobody resulted suffering from pathological depression according to our psychologist consultant (S.A). ED prevalence was 92.3% (12/13): 9 subjects with severe ED, 1 with moderate ED, and 2 with mild ED (the patient with localized AL was the only one not suffering from ED). The flowmetric indices showed a reduction of peak systolic value (PSV) in 76.9% of patients and a pathological acceleration (Acc) in 4/13. The population was analyzed based on both andrological and haematologic characteristics. Patients with pathological Acc showed a higher age (p=0.05) and worse scores at IIEF-TOT (p=0.006), at Desire Function (p=0.011), at Overall Satisfaction (p=0.034); patients with severe ED showed a higher age (p value = 0,003) and a pathological left Acc value (p value= 0,04); patients with mild ED and patient with normal erectile function (localized AL) showed normal right PSV (P value = 0,004) and normal left PSV (p value= 0,006) in comparison with patients with moderate and severe ED. Overall, no statistical difference was found for the two groups of patients: ED prevalence and ED stage was homogenous as the flowmetric characteristics. In the “off-therapy” group no differences were found according to hematologic response.
Conclusion
In our study a strong association between arterial inflow deficit, penile hemodynamic alteration, and ED was outlined. Having ruled out all possible causes for secondary ED, an arteriogenic cause, sustained by a possible cardiotoxic effect of extracellular light chain, was disclosed by the presence of early endothelial dysfunction in systemic AL patients independently of AL treatment received, time from AL diagnosis and organ involvement (the patient with localized AL was the only one not suffering from ED). A possible indication our study may provide is that any patient seeking medical advice for unexplained ED (common secondary ED causes ruled out) should undergo AL screening with QPE and FLC assay.
Keyword(s): Amyloidosis, Chemotherapy, Quality of life