

Contributions
Abstract: EP1160
Type: E-Poster Presentation
Session title: Platelet disorders
Background
Immune thrombocytopenia (ITP) is diagnosed in patients with a platelet (PLT) count below 100 x 109/L in whom other causes of thrombocytopenia have been ruled out. Myelodysplastic syndrome (MDS), aplastic anemia, myeloproliferative and lymphoproliferative diseases are among the main causes that are considered in the differential diagnosis.
Aims
As complete blood count (CBC) is one of the first tests that is performed on any patient who presents with clinical symptoms, our goal was to evaluate if standard and research CBC and reticulocyte parameters reported by Alinity hq can help differentiating ITP from other forms of thrombocytopenia.
Methods
The patient population (n=117) was selected to include samples with a PLT count of
< 100 x 109/L. The cohort included 38 unique samples from patients with ITP and 79 samples with other forms of thrombocytopenia, such as MDS, aplastic anemia, primary myelofibrosis and idiopathic cytopenia of undetermined significance, among others. CBC and reticulocyte results were generated with the Abbott Alinity hq hematology analyzer. Hematological parameters were compared between the two thrombocytopenic groups by the Mann-Whitney test. The effectiveness of standard and research CBC parameters and mathematical formulas to differentiate ITP for other forms of thrombocytopenia was assessed by ROC analysis. Patients who have received RBC transfusion in the past eight weeks were excluded from the analysis of RBC and reticulocyte parameters.
Results
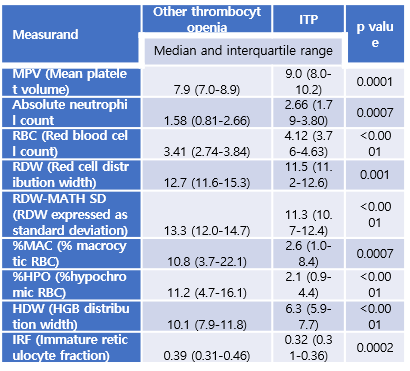
PLT counts were not significantly different between ITP and the other thrombocytopenia group (medians: 55.3 vs 46.9 x 109/L). Several CBC parameters demonstrated significant differences between the two populations.
The five parameters that showed the largest difference between the two groups (MPV, RBC, RDW-MATH SD, %HPO and HDW) produced area under the curve (AUC) values ranging from 0.676 (MPV) to 0.828 (HDW). Several mathematical formulas also demonstrated good performance. The formula of (RBC / HDW x MPV) resulted in an AUC of 0.848, and a sensitivity of 80.6% and specificity of 81.4% for differentiating ITP from other forms of thrombocytopenia.
Conclusion
Several Alinity hq standard and research CBC and reticulocyte parameters have demonstrated significant differences between ITP and other forms of thrombocytopenia. These differences are likely related to the fact that erythropoiesis and myelopoiesis are commonly affected in many forms of thrombocytopenia such as MDS or aplastic anemia, while they are not impacted in ITP. In addition, accelerated thrombopoiesis is present in ITP, but usually not in other types of thrombocytopenia. These results demonstrate the clinical utility of Alinity hq standard and research hematology parameters in the differential diagnosis of ITP.
Keyword(s): Thrombocytopenia
Abstract: EP1160
Type: E-Poster Presentation
Session title: Platelet disorders
Background
Immune thrombocytopenia (ITP) is diagnosed in patients with a platelet (PLT) count below 100 x 109/L in whom other causes of thrombocytopenia have been ruled out. Myelodysplastic syndrome (MDS), aplastic anemia, myeloproliferative and lymphoproliferative diseases are among the main causes that are considered in the differential diagnosis.
Aims
As complete blood count (CBC) is one of the first tests that is performed on any patient who presents with clinical symptoms, our goal was to evaluate if standard and research CBC and reticulocyte parameters reported by Alinity hq can help differentiating ITP from other forms of thrombocytopenia.
Methods
The patient population (n=117) was selected to include samples with a PLT count of
< 100 x 109/L. The cohort included 38 unique samples from patients with ITP and 79 samples with other forms of thrombocytopenia, such as MDS, aplastic anemia, primary myelofibrosis and idiopathic cytopenia of undetermined significance, among others. CBC and reticulocyte results were generated with the Abbott Alinity hq hematology analyzer. Hematological parameters were compared between the two thrombocytopenic groups by the Mann-Whitney test. The effectiveness of standard and research CBC parameters and mathematical formulas to differentiate ITP for other forms of thrombocytopenia was assessed by ROC analysis. Patients who have received RBC transfusion in the past eight weeks were excluded from the analysis of RBC and reticulocyte parameters.
Results
PLT counts were not significantly different between ITP and the other thrombocytopenia group (medians: 55.3 vs 46.9 x 109/L). Several CBC parameters demonstrated significant differences between the two populations.
The five parameters that showed the largest difference between the two groups (MPV, RBC, RDW-MATH SD, %HPO and HDW) produced area under the curve (AUC) values ranging from 0.676 (MPV) to 0.828 (HDW). Several mathematical formulas also demonstrated good performance. The formula of (RBC / HDW x MPV) resulted in an AUC of 0.848, and a sensitivity of 80.6% and specificity of 81.4% for differentiating ITP from other forms of thrombocytopenia.
Conclusion
Several Alinity hq standard and research CBC and reticulocyte parameters have demonstrated significant differences between ITP and other forms of thrombocytopenia. These differences are likely related to the fact that erythropoiesis and myelopoiesis are commonly affected in many forms of thrombocytopenia such as MDS or aplastic anemia, while they are not impacted in ITP. In addition, accelerated thrombopoiesis is present in ITP, but usually not in other types of thrombocytopenia. These results demonstrate the clinical utility of Alinity hq standard and research hematology parameters in the differential diagnosis of ITP.
Keyword(s): Thrombocytopenia