

Contributions
Abstract: EP1145
Type: E-Poster Presentation
Session title: Platelet disorders
Background
aTTP is an ultra-rare and potentially life-threatening thrombotic microangiopathy (TMA). Owing to the rarity of the disease, data on epidemiology, disease management, and clinical outcomes are scarce and often heterogeneous.
Aims
To assess the epidemiology, disease management, and clinical outcomes in patients with aTTP.
Methods
A longitudinal, retrospective observational study identified patients with an aTTP diagnosis from October 2015 to December 2019 in the Optum-Humedica database. Patients were eligible if they had ≥1 documented ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) test result <10% or ≥1 aTTP episode, defined as having ≥1 inpatient stay with an International Classification of Diseases (ICD) diagnosis of TMA (ICD, Ninth Revision [ICD-9], dx: 446.6; ICD, Tenth Revision [ICD-10], dx: M31.1) and ≥1 therapeutic plasma exchange (TPE) procedure (Current Procedural Terminology-4 code: 36514; ICD-10: 6A551Z3) during the same inpatient stay. Patients with a diagnosis of hemolytic uremic syndrome, Escherichia coli infection, human immunodeficiency virus, organ/stem cell transplant, systemic infection, and malignancy ≤6 months before or at index date were excluded. Index date was defined as the date of the earliest occurrence of an ADAMTS13 test result <10% or first TMA+TPE-related hospitalization during the study period. Index aTTP episode was defined as the first occurrence of TMA+TPE-related hospitalization. Patients were followed from the index date until the loss to follow-up, end of study period, or death, whichever occurred first. Incidence of aTTP, demographic, and clinical characteristics of patients, treatment patterns, and clinical outcomes were descriptively analyzed.
Results
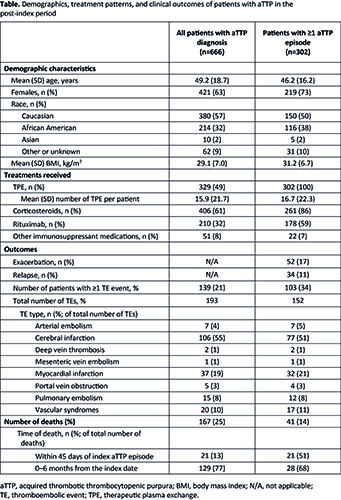
A total of 666 patients met inclusion criteria for aTTP diagnosis. Among these, 302 (45%) patients had ≥1 reported aTTP episode (TMA+TPE-related hospitalization). Patient demographics are summarized in the Table. The annual proportion of patients with documented aTTP (ADAMTS13 <10% or an aTTP episode) was 3.43/million, while the annual incidence of ≥1 aTTP episode was 1.81/million (averaged over 2016–2019).
Patients with ≥1 aTTP episode received a mean of 16.7 TPE sessions (standard deviation, 22.3); 86%, 59%, and 7% of patients received corticosteroids, rituximab, and other immunosuppressant treatments, respectively. The therapies received among all patients with aTTP diagnosis are summarized in the Table.
Exacerbations (rehospitalizations for TPE within the first 30 days following discharge for any aTTP episode) occurred in 17% (52/302) of patients with ≥1 episode. Relapse (new aTTP episode >30 days after discharge for the index episode) was reported in 11% (34/302) of these patients.
Mortality rate during follow-up among all patients with aTTP diagnosis was 25% (167/666), with 77% (129/167) of deaths occurring within 6 months of the index date. For patients with ≥1 aTTP episode, 14% (41/302) died, with 51% (21/41) of deaths occurring within 45 days of the index episode. Among all patients with aTTP diagnosis, 21% (139/666) of patients had ≥1 thromboembolic event (TE); of 193 total TEs reported, the most common were cerebral infarction (CI [55%]) and myocardial infarction (MI [19%]). For patients with ≥1 aTTP episode, 34% (103/302) had ≥1 TE; of the 152 TEs reported, CI (51%) and MI (21%) were the most common (Table).
Conclusion
Despite treatment with TPE and immunosuppressants, the high mortality and morbidity observed in this patient population demonstrates the need for more effective therapies to improve clinical outcomes.
Keyword(s): ADAMTS13, Thrombotic microangiopathy, Thrombotic thrombocytopenic purpura (TTP)
Abstract: EP1145
Type: E-Poster Presentation
Session title: Platelet disorders
Background
aTTP is an ultra-rare and potentially life-threatening thrombotic microangiopathy (TMA). Owing to the rarity of the disease, data on epidemiology, disease management, and clinical outcomes are scarce and often heterogeneous.
Aims
To assess the epidemiology, disease management, and clinical outcomes in patients with aTTP.
Methods
A longitudinal, retrospective observational study identified patients with an aTTP diagnosis from October 2015 to December 2019 in the Optum-Humedica database. Patients were eligible if they had ≥1 documented ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13) test result <10% or ≥1 aTTP episode, defined as having ≥1 inpatient stay with an International Classification of Diseases (ICD) diagnosis of TMA (ICD, Ninth Revision [ICD-9], dx: 446.6; ICD, Tenth Revision [ICD-10], dx: M31.1) and ≥1 therapeutic plasma exchange (TPE) procedure (Current Procedural Terminology-4 code: 36514; ICD-10: 6A551Z3) during the same inpatient stay. Patients with a diagnosis of hemolytic uremic syndrome, Escherichia coli infection, human immunodeficiency virus, organ/stem cell transplant, systemic infection, and malignancy ≤6 months before or at index date were excluded. Index date was defined as the date of the earliest occurrence of an ADAMTS13 test result <10% or first TMA+TPE-related hospitalization during the study period. Index aTTP episode was defined as the first occurrence of TMA+TPE-related hospitalization. Patients were followed from the index date until the loss to follow-up, end of study period, or death, whichever occurred first. Incidence of aTTP, demographic, and clinical characteristics of patients, treatment patterns, and clinical outcomes were descriptively analyzed.
Results
A total of 666 patients met inclusion criteria for aTTP diagnosis. Among these, 302 (45%) patients had ≥1 reported aTTP episode (TMA+TPE-related hospitalization). Patient demographics are summarized in the Table. The annual proportion of patients with documented aTTP (ADAMTS13 <10% or an aTTP episode) was 3.43/million, while the annual incidence of ≥1 aTTP episode was 1.81/million (averaged over 2016–2019).
Patients with ≥1 aTTP episode received a mean of 16.7 TPE sessions (standard deviation, 22.3); 86%, 59%, and 7% of patients received corticosteroids, rituximab, and other immunosuppressant treatments, respectively. The therapies received among all patients with aTTP diagnosis are summarized in the Table.
Exacerbations (rehospitalizations for TPE within the first 30 days following discharge for any aTTP episode) occurred in 17% (52/302) of patients with ≥1 episode. Relapse (new aTTP episode >30 days after discharge for the index episode) was reported in 11% (34/302) of these patients.
Mortality rate during follow-up among all patients with aTTP diagnosis was 25% (167/666), with 77% (129/167) of deaths occurring within 6 months of the index date. For patients with ≥1 aTTP episode, 14% (41/302) died, with 51% (21/41) of deaths occurring within 45 days of the index episode. Among all patients with aTTP diagnosis, 21% (139/666) of patients had ≥1 thromboembolic event (TE); of 193 total TEs reported, the most common were cerebral infarction (CI [55%]) and myocardial infarction (MI [19%]). For patients with ≥1 aTTP episode, 34% (103/302) had ≥1 TE; of the 152 TEs reported, CI (51%) and MI (21%) were the most common (Table).
Conclusion
Despite treatment with TPE and immunosuppressants, the high mortality and morbidity observed in this patient population demonstrates the need for more effective therapies to improve clinical outcomes.
Keyword(s): ADAMTS13, Thrombotic microangiopathy, Thrombotic thrombocytopenic purpura (TTP)