

Contributions
Abstract: EP1023
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Belantamab mafodotin (GSK2857916), an immuno-conjugate targeting B-cell maturation antigen, showed single-agent activity in the phase 1 and 2 studies in heavily pre-treated patients, and was recently approved for patients with relapsed/refractory multiple myeloma (RRMM) after 4 lines of therapy, including a proteosome inhibitor, immunomodulatory agent and an anti-CD38 monoclonal antibody. Real-world data and long-term follow-up are lacking.
Aims
To assess safety and efficacy of belantamb mafodotin therapy administered via the GSK expanded access compassionate care program for treatment of RRMM patients in a multi-site real-world setting.
Methods
All consecutive RRMM patients who received at least two doses of belantamab mafoditin under the expanded access compassionate care program in 9 Israeli centers were included. Data were extracted from medical charts focusing on demographics, disease characteristics, prior treatment, safety including ocular toxicity and disease responses. Primary endpoint was progression free survival (PFS), secondary endpoints included safety with focus on ocular toxicity, overall response rate (ORR), overall survival (OS), safety and tolerability.
Results
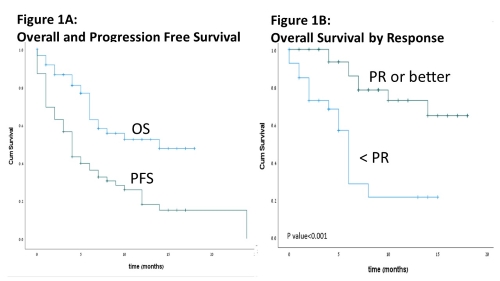
Sixty-seven RRMM patients, treated with belantamab mafodotin between July 2019 and February 2021 were included. Median follow-up was 16.1 (95% confidence interval [CI] 11.2-20.9) months. Median age was 70 (range 36-88) years. Forty-seven percent had a high-risk cytogenetic profile, including t(4;14), t(14;16), t(14;20), del17p and +1q). Patients were heavily pretreated with a median of 5 [IQR 4-7] prior therapy lines. Exposure rates to bortezomib, carfilzomib, lenalidomide, pomalidomide and daratumumab were 100%, 73%, 91%, 77% and 92%, respectively. Sixty-five percent and 23% were triple and penta- refractory, respectively. Median number of cycles was 4 (range 2-17) per patient. The maximal dose was 3.4 mg/kg and 2.5 mg/kg in 36% and in 56% of patients, respectively. Twenty-five percent (n=73) of the cycles beyond inital dose were delayed. Reasons for delays were mainly ocular toxicity (65%) followed by hematological (11%) toxicity and infections (5%). Ocular toxicity (keratopathy) occurred in 41 of 62 evaluable patients (66%). Worst ocular toxicity was grade 1, 2 and 3 in 10%, 23% and 32%, respectively. Resolution of grade ≥2 ocular toxicity to grade 1/0 was documented in 74% of the patients. Hematologic side effects included thrombocytopenia (39%, grade≥3: 31%), neutropenia (13%, grade≥3.9%) and anemia (9%, grade≥3.6%). Two grade 3 bleedings (epistaxis and upper gastrointestinal bleeding) were reported among patients with thrombocytopenia grade 3-4. Frequent non-hematologic adverse events included infection (10%, grade≥3: 6%) and elevation of liver enzymes (10%, grade≥3: 4%). Four patients (6%) discontinued therapy due to toxicity (ocular in all cases). ORR was 54%. Best response rates were: complete response, very good partial response, partial response, minor response, stable disease and progressive disease in 6%, 23%,25%,11%,14%, 20% of the patients, respectively. Median PFS was 4.4 (95% CI 3.3-5.5) months in the entire cohort and 8.8 (95% CI 6.2-11.3) months among responders (patients achieving PR or better, figure 1A). Median OS was 14 (95% CI NE) months. Among responders, median OS was not reached vs. 6 (95% CI 5.2-6.7) months in non-responders (p<0.001, figure 1B).
Conclusion
Belantamab mafodotin shows significant anti-myeloma activity in heavily pre-treated patients with RRMM in a real-world setting with a manageable safety profile.
Keyword(s): Multiple myeloma
Abstract: EP1023
Type: E-Poster Presentation
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Belantamab mafodotin (GSK2857916), an immuno-conjugate targeting B-cell maturation antigen, showed single-agent activity in the phase 1 and 2 studies in heavily pre-treated patients, and was recently approved for patients with relapsed/refractory multiple myeloma (RRMM) after 4 lines of therapy, including a proteosome inhibitor, immunomodulatory agent and an anti-CD38 monoclonal antibody. Real-world data and long-term follow-up are lacking.
Aims
To assess safety and efficacy of belantamb mafodotin therapy administered via the GSK expanded access compassionate care program for treatment of RRMM patients in a multi-site real-world setting.
Methods
All consecutive RRMM patients who received at least two doses of belantamab mafoditin under the expanded access compassionate care program in 9 Israeli centers were included. Data were extracted from medical charts focusing on demographics, disease characteristics, prior treatment, safety including ocular toxicity and disease responses. Primary endpoint was progression free survival (PFS), secondary endpoints included safety with focus on ocular toxicity, overall response rate (ORR), overall survival (OS), safety and tolerability.
Results
Sixty-seven RRMM patients, treated with belantamab mafodotin between July 2019 and February 2021 were included. Median follow-up was 16.1 (95% confidence interval [CI] 11.2-20.9) months. Median age was 70 (range 36-88) years. Forty-seven percent had a high-risk cytogenetic profile, including t(4;14), t(14;16), t(14;20), del17p and +1q). Patients were heavily pretreated with a median of 5 [IQR 4-7] prior therapy lines. Exposure rates to bortezomib, carfilzomib, lenalidomide, pomalidomide and daratumumab were 100%, 73%, 91%, 77% and 92%, respectively. Sixty-five percent and 23% were triple and penta- refractory, respectively. Median number of cycles was 4 (range 2-17) per patient. The maximal dose was 3.4 mg/kg and 2.5 mg/kg in 36% and in 56% of patients, respectively. Twenty-five percent (n=73) of the cycles beyond inital dose were delayed. Reasons for delays were mainly ocular toxicity (65%) followed by hematological (11%) toxicity and infections (5%). Ocular toxicity (keratopathy) occurred in 41 of 62 evaluable patients (66%). Worst ocular toxicity was grade 1, 2 and 3 in 10%, 23% and 32%, respectively. Resolution of grade ≥2 ocular toxicity to grade 1/0 was documented in 74% of the patients. Hematologic side effects included thrombocytopenia (39%, grade≥3: 31%), neutropenia (13%, grade≥3.9%) and anemia (9%, grade≥3.6%). Two grade 3 bleedings (epistaxis and upper gastrointestinal bleeding) were reported among patients with thrombocytopenia grade 3-4. Frequent non-hematologic adverse events included infection (10%, grade≥3: 6%) and elevation of liver enzymes (10%, grade≥3: 4%). Four patients (6%) discontinued therapy due to toxicity (ocular in all cases). ORR was 54%. Best response rates were: complete response, very good partial response, partial response, minor response, stable disease and progressive disease in 6%, 23%,25%,11%,14%, 20% of the patients, respectively. Median PFS was 4.4 (95% CI 3.3-5.5) months in the entire cohort and 8.8 (95% CI 6.2-11.3) months among responders (patients achieving PR or better, figure 1A). Median OS was 14 (95% CI NE) months. Among responders, median OS was not reached vs. 6 (95% CI 5.2-6.7) months in non-responders (p<0.001, figure 1B).
Conclusion
Belantamab mafodotin shows significant anti-myeloma activity in heavily pre-treated patients with RRMM in a real-world setting with a manageable safety profile.
Keyword(s): Multiple myeloma