

Contributions
Abstract: PB1787
Type: Publication Only
Session title: Stem cell transplantation - Clinical
Background
Therapeutic strategy for transplant-eligible NDMM patients (pts) is triplet-based induction scheme, with novel therapeutic agents (immunomodulators (IMIDs), proteasome inhibitors (IP) and even monoclonal antibodies as Daratumumab), to obtain better responses prior to conditioning regimen and TAPH. The standard of conditioning is MEL200. BORMEL200 vs MEL200 conditioning has been proposed, with better responses, similar toxicity, and prolonged progression-free survival (PFS) and overall survival (OS).
Aims
To analyse efficacy and toxicity depending on the administered conditioning: BORMEL200 vs MEL200 and VCd induction vs VTd / VRd.
Methods
Unicentric, descriptive and retrospective study carried out at Guadalajara University Hospital, from February 2010 to June 2020, using clinical and analytical NDMM pts data with ≥ partial response in the 1st line of treatment (tt). From February 2010 to July 2019, pts received BORMEL200: Bor sc (1mg/m2) days -6, -3, +1, +4 + MEL200 iv (200mg/m2) day -2, with G -CSF from day +7. From July 2019 to present, MEL200 iv, without G-CSF. In each conditioning, induction subgroups were analyzed: VCd vs VTd / VRd.
Results
We identified 61 pts whose clinical characteristics and treatment (tt) data are listed in Table 1. 48 (78,7%) received BORMEL200 and 13 (21,3%) MEL200. In general, pts received bortezomib (V) - based induction, of them 51% (n=31) were treated with alkylating agents and 49% (n=30) received immunomodulatory drugs.
In the group of BORMEL200, after a median follow-up of 9,7 years, the PFS and OS median for VCd and for VTd/VRd was 4,2 years and 9,7 years vs 4,7 years and not reached, respectively. In a PFS multivariable analysis, were included as independent variables: sex, age >65 years old, use of IMIDs (VTd/VRd), ISS, preTAPH response, high risk cytogenetic and infused CD34/kg quantity. It was associated independently to relapse: IMID use (HR 0.119; p = 0.003), age> 65 years (HR 0.832; p <0.001), ISS-2 vs ISS-1 (HR 62.2; p <0.001), ISS-3 vs ISS-1 (HR 36.3; p = 0.004).
In the MEL200 group, statistical data is not offered due to the few pts treated in both arms and short follow-up period.
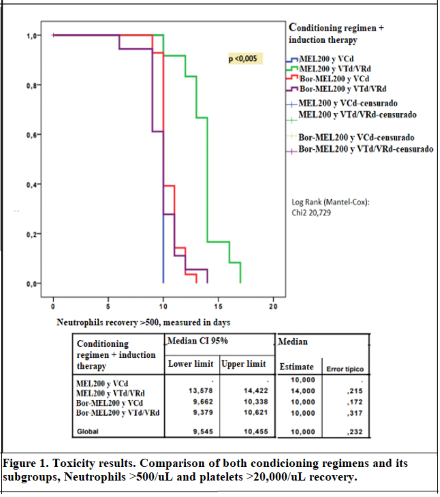
Regarding toxicity, the median of platelet recovery >20,000 was similar in both conditioning regimens. It was only found a significant association in the time till recovery neutrophils >500/ul, being superior in pts who received G-CSF during TAPH (Figure 1).
Conclusion
Among the patients with BORMEL200, the use of IMIDs does not provide better SLP in our series. BORMEL200 with VTd/VRd gets better postTAPH responses. An early recovery of neutrophils in conditioning with G-CSF is observed, with the clinical and socioeconomic implications associated. More patients need to be included in both treatment branches and a better follow-up and monitoring so that data may be confirmed.
Keyword(s): Autologous bone marrow transplant, Complications, Conditioning, Multiple myeloma
Abstract: PB1787
Type: Publication Only
Session title: Stem cell transplantation - Clinical
Background
Therapeutic strategy for transplant-eligible NDMM patients (pts) is triplet-based induction scheme, with novel therapeutic agents (immunomodulators (IMIDs), proteasome inhibitors (IP) and even monoclonal antibodies as Daratumumab), to obtain better responses prior to conditioning regimen and TAPH. The standard of conditioning is MEL200. BORMEL200 vs MEL200 conditioning has been proposed, with better responses, similar toxicity, and prolonged progression-free survival (PFS) and overall survival (OS).
Aims
To analyse efficacy and toxicity depending on the administered conditioning: BORMEL200 vs MEL200 and VCd induction vs VTd / VRd.
Methods
Unicentric, descriptive and retrospective study carried out at Guadalajara University Hospital, from February 2010 to June 2020, using clinical and analytical NDMM pts data with ≥ partial response in the 1st line of treatment (tt). From February 2010 to July 2019, pts received BORMEL200: Bor sc (1mg/m2) days -6, -3, +1, +4 + MEL200 iv (200mg/m2) day -2, with G -CSF from day +7. From July 2019 to present, MEL200 iv, without G-CSF. In each conditioning, induction subgroups were analyzed: VCd vs VTd / VRd.
Results
We identified 61 pts whose clinical characteristics and treatment (tt) data are listed in Table 1. 48 (78,7%) received BORMEL200 and 13 (21,3%) MEL200. In general, pts received bortezomib (V) - based induction, of them 51% (n=31) were treated with alkylating agents and 49% (n=30) received immunomodulatory drugs.
In the group of BORMEL200, after a median follow-up of 9,7 years, the PFS and OS median for VCd and for VTd/VRd was 4,2 years and 9,7 years vs 4,7 years and not reached, respectively. In a PFS multivariable analysis, were included as independent variables: sex, age >65 years old, use of IMIDs (VTd/VRd), ISS, preTAPH response, high risk cytogenetic and infused CD34/kg quantity. It was associated independently to relapse: IMID use (HR 0.119; p = 0.003), age> 65 years (HR 0.832; p <0.001), ISS-2 vs ISS-1 (HR 62.2; p <0.001), ISS-3 vs ISS-1 (HR 36.3; p = 0.004).
In the MEL200 group, statistical data is not offered due to the few pts treated in both arms and short follow-up period.
Regarding toxicity, the median of platelet recovery >20,000 was similar in both conditioning regimens. It was only found a significant association in the time till recovery neutrophils >500/ul, being superior in pts who received G-CSF during TAPH (Figure 1).
Conclusion
Among the patients with BORMEL200, the use of IMIDs does not provide better SLP in our series. BORMEL200 with VTd/VRd gets better postTAPH responses. An early recovery of neutrophils in conditioning with G-CSF is observed, with the clinical and socioeconomic implications associated. More patients need to be included in both treatment branches and a better follow-up and monitoring so that data may be confirmed.
Keyword(s): Autologous bone marrow transplant, Complications, Conditioning, Multiple myeloma