

Contributions
Abstract: PB1778
Type: Publication Only
Session title: Stem cell transplantation - Clinical
Background
Hepatic sinusoidal obstruction syndrome (SOS) is one of the complications of allogeneic stem cell transplantation (allo-SCT) due to endothelial dysfunction. Defibrotide (DF) is used effectively in SOS prophylaxis and treatment because of its endothelial protective and thrombocytic-fibrinolytic regulatory effects . On the other hand, graft versus host disease (GVHD), regardless of whether acute chronic or overlap syndrome, is the most important cause of morbidity and mortality in ASCT.
Aims
Here, we retrospectively investigated the use of DF and its effect on the development of GVHD in our allogeneic transplant patients.
Methods
Eighty-one patients with various diagnoses (including myeloid and lymphoid hematological malignancies and aplastic anemia), who underwent allo-SCT at the Hematology Department of Adnan Menderes University between 2014-2020 were included. Of the patients, 34 used DF as a prophylaxis (25mg/kg/day, intravenously, 21 days) while 47 patients did not. Acute and chronic GVHD and overlap syndrome assessment were performed at +30/100th day and throughout the life of the patient, respectively. The data were evaluated using SPSS 21 software program (Chicago, IL, USA). Chi-square test was used to demonstrate the difference between categorical variables. A p value below 0, 05 was the cutoff for statistical significance.
Results
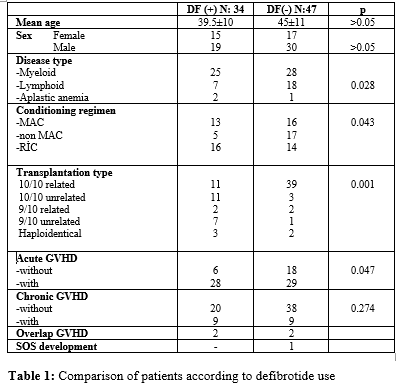
The results for the patients are presented in Table 1. Thirteen patients (38%) in the DF group and 16 patients (34%) in the non-DF group received myeloablative conditioning regimens containing busulfan. The rest of the patients in both groups received non-myeloablative or reduced intensity conditioning regimens. Acute GVHD was more common in patients who received DF, compared to patients who did not receive it (82% vs 61%). Although rates of chronic GVHD differ among DF users compared to non-users (31% vs 19%); it did not reach a statistically significant value (p: 0,274). While no patient died in the group that did not use DF, 5 patients died in the first 100 days in the group using DF. Overlap GVHD was observed in 4 patients. We observed that 1 patient in the non-DF group developed SOS according to the European Bone Marrow Transplantation (EBMT) criteria.
Conclusion
In our study, DF use was evaluated in terms of the development of acute and chronic GVHD and we noted the development of more acute GVHD with the use of DF. There was no difference in the development of chronic GVHD. There are few studies in the literature evaluating the relationship between DF use and GVHD. In an in vitro study on mice, DF use was shown to be effective in acute GVHD through T lymphocyte and neutrophil interaction. In another experimental study, it was shown to suppress acute GVHD by inhibiting the 'endothelial cell line' activation. In contrast to our study, acute GVHD was less common in another clinical study by Tekgündüz et al (46, 5% vs 82%). To the best of our knowledge, this is the first study evaluating the effect of DF on both acute and chronic GVHD in the adult population. The use of DF for prophylaxis is mostly preferred in high risk patients. Development of GVHD is also important for this risk group. These risks may explain the higher rate of acute GVHD in the DF group in our study. The effects of DF use on GVHD will be clarified with studies in which both the use of DF and risk subgroups of GVHD development are evaluated using a high and homogeneous number of patients.
Keyword(s): Defibrotide, Graft-versus-host disease (GVHD)
Abstract: PB1778
Type: Publication Only
Session title: Stem cell transplantation - Clinical
Background
Hepatic sinusoidal obstruction syndrome (SOS) is one of the complications of allogeneic stem cell transplantation (allo-SCT) due to endothelial dysfunction. Defibrotide (DF) is used effectively in SOS prophylaxis and treatment because of its endothelial protective and thrombocytic-fibrinolytic regulatory effects . On the other hand, graft versus host disease (GVHD), regardless of whether acute chronic or overlap syndrome, is the most important cause of morbidity and mortality in ASCT.
Aims
Here, we retrospectively investigated the use of DF and its effect on the development of GVHD in our allogeneic transplant patients.
Methods
Eighty-one patients with various diagnoses (including myeloid and lymphoid hematological malignancies and aplastic anemia), who underwent allo-SCT at the Hematology Department of Adnan Menderes University between 2014-2020 were included. Of the patients, 34 used DF as a prophylaxis (25mg/kg/day, intravenously, 21 days) while 47 patients did not. Acute and chronic GVHD and overlap syndrome assessment were performed at +30/100th day and throughout the life of the patient, respectively. The data were evaluated using SPSS 21 software program (Chicago, IL, USA). Chi-square test was used to demonstrate the difference between categorical variables. A p value below 0, 05 was the cutoff for statistical significance.
Results
The results for the patients are presented in Table 1. Thirteen patients (38%) in the DF group and 16 patients (34%) in the non-DF group received myeloablative conditioning regimens containing busulfan. The rest of the patients in both groups received non-myeloablative or reduced intensity conditioning regimens. Acute GVHD was more common in patients who received DF, compared to patients who did not receive it (82% vs 61%). Although rates of chronic GVHD differ among DF users compared to non-users (31% vs 19%); it did not reach a statistically significant value (p: 0,274). While no patient died in the group that did not use DF, 5 patients died in the first 100 days in the group using DF. Overlap GVHD was observed in 4 patients. We observed that 1 patient in the non-DF group developed SOS according to the European Bone Marrow Transplantation (EBMT) criteria.
Conclusion
In our study, DF use was evaluated in terms of the development of acute and chronic GVHD and we noted the development of more acute GVHD with the use of DF. There was no difference in the development of chronic GVHD. There are few studies in the literature evaluating the relationship between DF use and GVHD. In an in vitro study on mice, DF use was shown to be effective in acute GVHD through T lymphocyte and neutrophil interaction. In another experimental study, it was shown to suppress acute GVHD by inhibiting the 'endothelial cell line' activation. In contrast to our study, acute GVHD was less common in another clinical study by Tekgündüz et al (46, 5% vs 82%). To the best of our knowledge, this is the first study evaluating the effect of DF on both acute and chronic GVHD in the adult population. The use of DF for prophylaxis is mostly preferred in high risk patients. Development of GVHD is also important for this risk group. These risks may explain the higher rate of acute GVHD in the DF group in our study. The effects of DF use on GVHD will be clarified with studies in which both the use of DF and risk subgroups of GVHD development are evaluated using a high and homogeneous number of patients.
Keyword(s): Defibrotide, Graft-versus-host disease (GVHD)