

Contributions
Abstract: PB1771
Type: Publication Only
Session title: Sickle cell disease
Background
A strong association between pancreatic iron burden and cardiac complications was found in patients with thalassemia major. There is no study evaluating this issue in sickle cell disease (SCD).
Aims
The objective of this multicenter study was to systematically explore the link between pancreatic iron and cardiovascular complications in a cohort SCD patients enrolled at baseline in the prospective Extension-Myocardial Iron Overload in Thalassaemia (E-MIOT) project.
Methods
We considered consecutively enrolled 63 patients: 44 with sickle beta thalassemia, 18 with sickle cell anemia (SCA), and one with hemoglobin SC disease (HbSC). Mean age was 36.6±14.4 years and 29 patients were females. T2* measurements were performed over pancreatic head, body and tail and global value was the mean. Myocardial iron overload (MIO) was quantified using a T2* segmental approach.
Results
SCA and sickle beta thalassemia patients were comparable for age, sex, hematochemical parameters, and cardiac and pancreatic T2* values.
Transfusion dependent (TD; N=44) and no-TD patients showed comparable global pancreas T2* values (29.8±11.4 ms vs 32.2±8.0 ms; P=0.414), but were more frequently chelated (79.1% vs 52.6%; P=0.034).
Nineteen patients (30.2%) showed a pathological global pancreas T2* value (<26 ms) while no patient had significant myocardial iron overload (global heart T2*<20 ms).
Seven patients (11.1%) had at least one cardiovascular complication: two supraventricular arrhythmias, one heart failure, one heart failure + pulmonary hypertension, one myocardial infarction, one deep vein thrombosis, and one leg ulcer. Frequency of cardiovascular complications was comparable among the forms of SCD, but all complications occurred in regularly transfused patients.
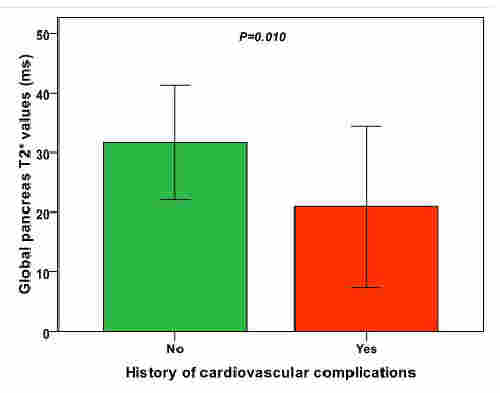
Patients with cardiovascular complications showed significantly lower global pancreas T2* values than patients free of cardiovascular complications (20.9±13.5 ms vs 31.7±9.6 ms; P=0.010) (Figure 1) but comparable global heart T2* values (38.4±5.6 ms vs 40.6±4.7 ms; P=0.257). Patients with pancreatic iron overload were more likely to have cardiovascular complications [odds ratio=7.5 (95%confidence intervals=1.3-43.1); P=0.024].
Conclusion
Pancreatic iron overload is associated with an increased risk of cardiovascular complications in SCD patients. If a patient has pancreatic iron overload, it would be prudent to start or intensify iron chelation therapy to prospectively prevent cardiac damage.
Keyword(s): Iron overload, Pancreas, Sickle cell disease
Abstract: PB1771
Type: Publication Only
Session title: Sickle cell disease
Background
A strong association between pancreatic iron burden and cardiac complications was found in patients with thalassemia major. There is no study evaluating this issue in sickle cell disease (SCD).
Aims
The objective of this multicenter study was to systematically explore the link between pancreatic iron and cardiovascular complications in a cohort SCD patients enrolled at baseline in the prospective Extension-Myocardial Iron Overload in Thalassaemia (E-MIOT) project.
Methods
We considered consecutively enrolled 63 patients: 44 with sickle beta thalassemia, 18 with sickle cell anemia (SCA), and one with hemoglobin SC disease (HbSC). Mean age was 36.6±14.4 years and 29 patients were females. T2* measurements were performed over pancreatic head, body and tail and global value was the mean. Myocardial iron overload (MIO) was quantified using a T2* segmental approach.
Results
SCA and sickle beta thalassemia patients were comparable for age, sex, hematochemical parameters, and cardiac and pancreatic T2* values.
Transfusion dependent (TD; N=44) and no-TD patients showed comparable global pancreas T2* values (29.8±11.4 ms vs 32.2±8.0 ms; P=0.414), but were more frequently chelated (79.1% vs 52.6%; P=0.034).
Nineteen patients (30.2%) showed a pathological global pancreas T2* value (<26 ms) while no patient had significant myocardial iron overload (global heart T2*<20 ms).
Seven patients (11.1%) had at least one cardiovascular complication: two supraventricular arrhythmias, one heart failure, one heart failure + pulmonary hypertension, one myocardial infarction, one deep vein thrombosis, and one leg ulcer. Frequency of cardiovascular complications was comparable among the forms of SCD, but all complications occurred in regularly transfused patients.
Patients with cardiovascular complications showed significantly lower global pancreas T2* values than patients free of cardiovascular complications (20.9±13.5 ms vs 31.7±9.6 ms; P=0.010) (Figure 1) but comparable global heart T2* values (38.4±5.6 ms vs 40.6±4.7 ms; P=0.257). Patients with pancreatic iron overload were more likely to have cardiovascular complications [odds ratio=7.5 (95%confidence intervals=1.3-43.1); P=0.024].
Conclusion
Pancreatic iron overload is associated with an increased risk of cardiovascular complications in SCD patients. If a patient has pancreatic iron overload, it would be prudent to start or intensify iron chelation therapy to prospectively prevent cardiac damage.
Keyword(s): Iron overload, Pancreas, Sickle cell disease