

Contributions
Abstract: PB1651
Type: Publication Only
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Multiple myeloma (MM) is a bone marrow neoplasm that accounts for 1% of all cancers. Besides, it also constitutes a 10% of haematological malignancies. Nowadays, MM continues to be an incurable disease that affects the elderly. It is not a well-known disease by general practitioners and its symptoms are also common in many other conditions which make it difficult to suspect MM as the underlying cause. Longer time to diagnosis is associated with more complications and irretrievable consequences.
Aims
Assessing the delay in the diagnosis of MM, number of visits in different health units, reasons for consultation and possible consequences.
Methods
We have carried out a retrospective study and we have analysed all new diagnoses of MM patients between 1st January 2017 and 31th December 2020 in our centre. Patients with monoclonal gammopathy of undetermined significance (MGUS), previous or another centre diagnosis were excluded. We define “delay in diagnosis” as the time that elapses from the first consultation of the patient for any symptom or sign related to the disease until the final diagnosis of MM by bone marrow aspiration.
Results
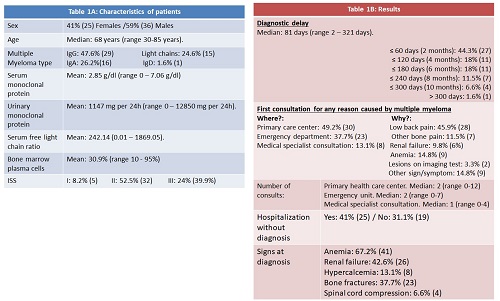
In total, 61 patients were diagnosed as de novo MM, between 2017 and 2020. Median age was 68 years (range 30-85 years). 41% (25 patients) were females and 59% (36) were males. IgG was the most frequent type of MM (47.5%) and more than a half of patients were stage two by MM international staging system (ISS). Characteristics of patients are in table 1A and the results of sample in table 1B.
The average delay in diagnosis was 81 days (range 2-321 days) and in 27 patients (44.3%) the retardation between the first claim for a MM symptom and diagnosis was equal or less than 60 days. However, 11 patients (18%) were diagnosed within more than two months and equal or less than four months and the delay was more than 120 days in 23 patients (37.7%). Besides, almost 20% of patients waited for more than 6 months to be diagnosed.
The first consultation for any sign or symptom was in primary care centres (49.2%), emergency services (37.7%) or another specialist hospital consultation (17%) and low back pain was the reason in almost half of the patients (45.9%).
Two visits (range 0-12) were the median in care centres but 40.9% of patients needed more than two and 9 people (14.7%) went more than five times. Also, the median was two visits (range 0-7) in emergencies, although 42.5% of patients were three times or more. In consultation with another specialist (nephrology, traumatology, internal medicine…) median of visits was one (range 0-4).
Twenty-five patients (41%) were admitted without diagnosis to the hospital by internal medicine. At diagnosis, anemia was presented in 67.2% of patients, kidney failure in 42.6%, hyperkalaemia in 13.1%, bone fractures in 37.7% and 6.6% of patients had spinal cord compression.
Conclusion
We believe that there is a significant delay in the diagnosis of patients with MM. There are probably many reasons for this, but we think that one of the most important is the lack of knowledge about this pathology outside the haematology units. Based on these data, we are going to implement a protocol for the early diagnosis of myeloma, in collaboration with the emergency department, other hospital specialties and the primary care centres in our health area. The protocol is already written and it is approved by the hospital's medical management. With the implementation of the protocol, our objective is to reduce the delay in the diagnosis of these type of patients.
Keyword(s): Diagnosis, Multiple myeloma
Abstract: PB1651
Type: Publication Only
Session title: Myeloma and other monoclonal gammopathies - Clinical
Background
Multiple myeloma (MM) is a bone marrow neoplasm that accounts for 1% of all cancers. Besides, it also constitutes a 10% of haematological malignancies. Nowadays, MM continues to be an incurable disease that affects the elderly. It is not a well-known disease by general practitioners and its symptoms are also common in many other conditions which make it difficult to suspect MM as the underlying cause. Longer time to diagnosis is associated with more complications and irretrievable consequences.
Aims
Assessing the delay in the diagnosis of MM, number of visits in different health units, reasons for consultation and possible consequences.
Methods
We have carried out a retrospective study and we have analysed all new diagnoses of MM patients between 1st January 2017 and 31th December 2020 in our centre. Patients with monoclonal gammopathy of undetermined significance (MGUS), previous or another centre diagnosis were excluded. We define “delay in diagnosis” as the time that elapses from the first consultation of the patient for any symptom or sign related to the disease until the final diagnosis of MM by bone marrow aspiration.
Results
In total, 61 patients were diagnosed as de novo MM, between 2017 and 2020. Median age was 68 years (range 30-85 years). 41% (25 patients) were females and 59% (36) were males. IgG was the most frequent type of MM (47.5%) and more than a half of patients were stage two by MM international staging system (ISS). Characteristics of patients are in table 1A and the results of sample in table 1B.
The average delay in diagnosis was 81 days (range 2-321 days) and in 27 patients (44.3%) the retardation between the first claim for a MM symptom and diagnosis was equal or less than 60 days. However, 11 patients (18%) were diagnosed within more than two months and equal or less than four months and the delay was more than 120 days in 23 patients (37.7%). Besides, almost 20% of patients waited for more than 6 months to be diagnosed.
The first consultation for any sign or symptom was in primary care centres (49.2%), emergency services (37.7%) or another specialist hospital consultation (17%) and low back pain was the reason in almost half of the patients (45.9%).
Two visits (range 0-12) were the median in care centres but 40.9% of patients needed more than two and 9 people (14.7%) went more than five times. Also, the median was two visits (range 0-7) in emergencies, although 42.5% of patients were three times or more. In consultation with another specialist (nephrology, traumatology, internal medicine…) median of visits was one (range 0-4).
Twenty-five patients (41%) were admitted without diagnosis to the hospital by internal medicine. At diagnosis, anemia was presented in 67.2% of patients, kidney failure in 42.6%, hyperkalaemia in 13.1%, bone fractures in 37.7% and 6.6% of patients had spinal cord compression.
Conclusion
We believe that there is a significant delay in the diagnosis of patients with MM. There are probably many reasons for this, but we think that one of the most important is the lack of knowledge about this pathology outside the haematology units. Based on these data, we are going to implement a protocol for the early diagnosis of myeloma, in collaboration with the emergency department, other hospital specialties and the primary care centres in our health area. The protocol is already written and it is approved by the hospital's medical management. With the implementation of the protocol, our objective is to reduce the delay in the diagnosis of these type of patients.
Keyword(s): Diagnosis, Multiple myeloma