

Contributions
Abstract: PB1638
Type: Publication Only
Session title: Myeloma and other monoclonal gammopathies - Biology & Translational Research
Background
C-reactive protein (CRP) is the most used clinical indicator of inflammation, which under certain circumstances can dissociate into insoluble monomers (mCRP). A recent study identified that mCRP can increase the number of osteoclasts in the culture medium. It is known that osteolytic lesions are a hallmark of MM, causing severe bone pain and pathological fractures. The malignant plasma cells induce bone resorption by activating osteoclasts. On the other hand, a Renal impairment (RI) is others common in MM)], with up to 40% of the patients experiencing this complication. RI increases risk of early death and affects disease management in multiple ways, as it may complicate treatment options and dosing, and render pts more susceptible to infections and prolonged hospitalizations. In addition, in the case of RI, traditional prognostic markers such as albumin and beta2-microglobulin are less accurate in terms of disease prevalence and tumor volume.
Aims
The target was to study the importance of mCRP as a marker of bone resorption for this kind of patients.
Methods
Blood samples were collected from patients before starting chemotherapy. To distinguish between mCRP and pentameric CRP, we combined the FITC-labeled monoclonal antibody to pCRP (mAb to pCRP), clone 372 (ImTek, Moscow, Russia), and PE-labeled mAb to mCRP with cross-reactivity to pCRP (mAb to mCRP), clone 328 (ImTek, Moscow, Russia). We used a non-specific FITC-labeled mouse IgG as a negative control. In each test at least 10,000 events were registered. We prospectively evaluated 15 patients with newly diagnosed MM (median age at diagnosis 67 years, range 55-74 years, female-9/male-6). A feature of our population of patients was a severe renal failure with a median of CKD-EPI 6.3 [Q25 5.2; Q75 12.3] ml/min/1.73 m2.
Results
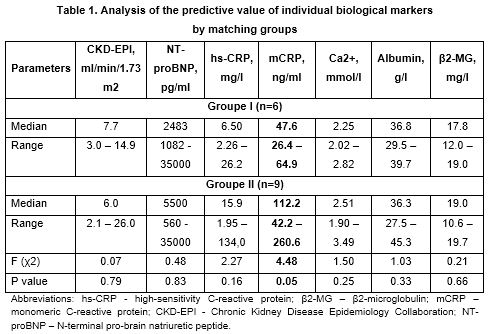
The degree of bone destruction was assessed using X-ray, based on which, the patients were divided into 2 groups. For patients with limited bone loss (corresponds to stages Durie-Salmon 1-2, Groupe I, n=6), the median of mCRP was 47.6 [35.3; 62.5] versus 112.6 [75.6; 183.2] ng/ml (p = 0.02) for advanced lytic bone lesions (DS stage 3, Groupe B, n=9). This is much more than healthy people who have an mCRP level of 1 ng/ml. Only the concentration of mCRP, but not CRP, Ca2+, albumin, β2-microglobulin or NT-proBNP, correlated with bone destruction (Table 1).
Conclusion
Thus, we concluded that there is a relationship between the degree of bone destruction and mCRP concentration. Hence mCRP plays an important role in the increase in the number of osteoclasts and increasing their activity, it can serve as a good marker of bone resorption.
Keyword(s): Bone disease, Multiple myeloma, Prognostic factor
Abstract: PB1638
Type: Publication Only
Session title: Myeloma and other monoclonal gammopathies - Biology & Translational Research
Background
C-reactive protein (CRP) is the most used clinical indicator of inflammation, which under certain circumstances can dissociate into insoluble monomers (mCRP). A recent study identified that mCRP can increase the number of osteoclasts in the culture medium. It is known that osteolytic lesions are a hallmark of MM, causing severe bone pain and pathological fractures. The malignant plasma cells induce bone resorption by activating osteoclasts. On the other hand, a Renal impairment (RI) is others common in MM)], with up to 40% of the patients experiencing this complication. RI increases risk of early death and affects disease management in multiple ways, as it may complicate treatment options and dosing, and render pts more susceptible to infections and prolonged hospitalizations. In addition, in the case of RI, traditional prognostic markers such as albumin and beta2-microglobulin are less accurate in terms of disease prevalence and tumor volume.
Aims
The target was to study the importance of mCRP as a marker of bone resorption for this kind of patients.
Methods
Blood samples were collected from patients before starting chemotherapy. To distinguish between mCRP and pentameric CRP, we combined the FITC-labeled monoclonal antibody to pCRP (mAb to pCRP), clone 372 (ImTek, Moscow, Russia), and PE-labeled mAb to mCRP with cross-reactivity to pCRP (mAb to mCRP), clone 328 (ImTek, Moscow, Russia). We used a non-specific FITC-labeled mouse IgG as a negative control. In each test at least 10,000 events were registered. We prospectively evaluated 15 patients with newly diagnosed MM (median age at diagnosis 67 years, range 55-74 years, female-9/male-6). A feature of our population of patients was a severe renal failure with a median of CKD-EPI 6.3 [Q25 5.2; Q75 12.3] ml/min/1.73 m2.
Results
The degree of bone destruction was assessed using X-ray, based on which, the patients were divided into 2 groups. For patients with limited bone loss (corresponds to stages Durie-Salmon 1-2, Groupe I, n=6), the median of mCRP was 47.6 [35.3; 62.5] versus 112.6 [75.6; 183.2] ng/ml (p = 0.02) for advanced lytic bone lesions (DS stage 3, Groupe B, n=9). This is much more than healthy people who have an mCRP level of 1 ng/ml. Only the concentration of mCRP, but not CRP, Ca2+, albumin, β2-microglobulin or NT-proBNP, correlated with bone destruction (Table 1).
Conclusion
Thus, we concluded that there is a relationship between the degree of bone destruction and mCRP concentration. Hence mCRP plays an important role in the increase in the number of osteoclasts and increasing their activity, it can serve as a good marker of bone resorption.
Keyword(s): Bone disease, Multiple myeloma, Prognostic factor