

Contributions
Abstract: PB1492
Type: Publication Only
Session title: Chronic lymphocytic leukemia and related disorders - Clinical
Background
Large granular lymphocyte leukemia (LGLL)-associated pure red cell aplasia (PRCA) is a rare lymphoproliferative disorder. Only a few case series have been reported in the literature. so that the features and optimal treatment of the disease remains unclear.
Aims
We conducted this retrospective study to assess clinical features, immunological profiles and the outcome of treatment in patients with LGLL-associated PRCA.
Methods
A cohort of 20 patients with LGLL-associated PRCA who referred to our hospital from January 2013 to April 2020 was reviewed.
Results
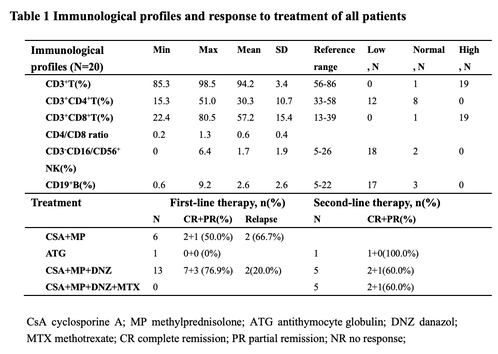
The clinical characteristics of 20 patients included in this study showed that no differences were evident based on sex. The median age of the patients was 50 years old (range, 28-76 years). Splenomegaly was observed in 45% of cases, most of which were characterized by mild to moderate enlargement. By contrast, hepatomegaly was rare (10%). Our study identified increased percentage and absolute number of CD3+CD8+ T cells, meanwhile decreased CD3+CD4+ T cells,CD3−CD16/CD56+ NK,CD19+ B cells and CD4/CD8 ratio (Table 1). For treatment (Table 1), cyclosporine A (CSA) in combination with methylprednisolone (MP) was administered in 6 patients, with an complete and partial remission (CR+PR) of 50.0% (3/6). A novel immunosuppressive strategy of cyclosporine (CSA), low dose methylprednisolone (MP) and danazol(DNZ), which we named CMD regimen, was administrated orally with an initial dose of CSA 3mg/kg/day , MP 0.25−0.5 mg/kg/day, and DNZ 5.0-10.0 mg/kg daily as first-line therapy for 13 patients, of which ten responded positively(76.9%). One patient received antithymocyte globulin (ATG), resulting in no response (NR). Among the three patients who failed to respond and two relapse to first-line therapy of CSA and MP , four patients received the second-line therapy of CMD regimen, with an CR+PR of 60%. Another patient received ATG, and achieved complete remission (CR). Among the three patients who failed to respond and two relapse to first-line therapy of CMD regimen, three patient responded to the second-line therapy of CMD regimen plus methotrexate (MTX). Adverse events were uncommon, one patient had impairment of liver function with transaminase values up to 110 U/L.
Conclusion
This study provides new information regarding the clinical features and therapeutic strategies for LGLL-associated PRCA, which demonstrated that the CMD regimen could be a promising strategy for patients with LGLL-associated PRCA.The multiple-center clinical trial need to initiate to validate this conclusion.
Keyword(s): Large granular lymphocytic leukaemia, Pure red cell aplasia
Abstract: PB1492
Type: Publication Only
Session title: Chronic lymphocytic leukemia and related disorders - Clinical
Background
Large granular lymphocyte leukemia (LGLL)-associated pure red cell aplasia (PRCA) is a rare lymphoproliferative disorder. Only a few case series have been reported in the literature. so that the features and optimal treatment of the disease remains unclear.
Aims
We conducted this retrospective study to assess clinical features, immunological profiles and the outcome of treatment in patients with LGLL-associated PRCA.
Methods
A cohort of 20 patients with LGLL-associated PRCA who referred to our hospital from January 2013 to April 2020 was reviewed.
Results
The clinical characteristics of 20 patients included in this study showed that no differences were evident based on sex. The median age of the patients was 50 years old (range, 28-76 years). Splenomegaly was observed in 45% of cases, most of which were characterized by mild to moderate enlargement. By contrast, hepatomegaly was rare (10%). Our study identified increased percentage and absolute number of CD3+CD8+ T cells, meanwhile decreased CD3+CD4+ T cells,CD3−CD16/CD56+ NK,CD19+ B cells and CD4/CD8 ratio (Table 1). For treatment (Table 1), cyclosporine A (CSA) in combination with methylprednisolone (MP) was administered in 6 patients, with an complete and partial remission (CR+PR) of 50.0% (3/6). A novel immunosuppressive strategy of cyclosporine (CSA), low dose methylprednisolone (MP) and danazol(DNZ), which we named CMD regimen, was administrated orally with an initial dose of CSA 3mg/kg/day , MP 0.25−0.5 mg/kg/day, and DNZ 5.0-10.0 mg/kg daily as first-line therapy for 13 patients, of which ten responded positively(76.9%). One patient received antithymocyte globulin (ATG), resulting in no response (NR). Among the three patients who failed to respond and two relapse to first-line therapy of CSA and MP , four patients received the second-line therapy of CMD regimen, with an CR+PR of 60%. Another patient received ATG, and achieved complete remission (CR). Among the three patients who failed to respond and two relapse to first-line therapy of CMD regimen, three patient responded to the second-line therapy of CMD regimen plus methotrexate (MTX). Adverse events were uncommon, one patient had impairment of liver function with transaminase values up to 110 U/L.
Conclusion
This study provides new information regarding the clinical features and therapeutic strategies for LGLL-associated PRCA, which demonstrated that the CMD regimen could be a promising strategy for patients with LGLL-associated PRCA.The multiple-center clinical trial need to initiate to validate this conclusion.
Keyword(s): Large granular lymphocytic leukaemia, Pure red cell aplasia