

Contributions
Abstract: PB1398
Type: Publication Only
Session title: Acute myeloid leukemia - Clinical
Background
In older patients (pts) with acute myeloid leukemia (AML), intensive chemotherapy can induce complete remission, but responses are often short and overall survival (OS) is poor after relapse. Azacitadine (AZA) maintenance therapies (MT) may improve disease-free survival in pts aged ≥60 years, but have not been shown to improve OS (Oliva EN, et al. ASH 2019; Huls G, et al. Blood 2019). In addition, AZA is given subcutaneously or intravenously (IV), resulting in a high administration burden and potential for infusion reactions. In the phase 3 QUAZAR AML-001 study, a novel oral formulation of AZA was the first MT to show a significant and clinically meaningful improvement in both OS and relapse-free survival (Wei AH, et al. N Engl J Med 2020). While oral AZA offers an effective MT option, little is known about the treatment preferences of pts with AML. We conducted a discrete choice experiment (DCE) survey of pts aged ≥55 years with AML in the USA, Canada, Germany, and Italy to assess the relative importance of key attributes of MT options (Tervonen T, et al. ASH 2020). Globally, pts placed the highest importance on survival probability at 2 years and were willing to accept reduced efficacy for the convenience of oral administration; this subgroup analysis explored the importance that pts in Germany and Italy placed on key factors.
Aims
To examine the relative importance of key attributes of MT among a subgroup of pts aged ≥55 years with AML from Germany and Italy.
Methods
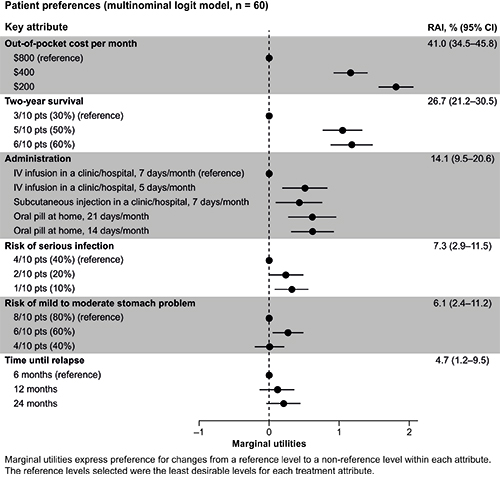
An online DCE was conducted in the USA, Canada, Germany, and Italy between November 2019 and April 2020 to identify preferences for MT attributes among pts aged ≥55 years with AML. DCE data were analyzed using a multinomial logit (MNL) model. The MNL model estimated marginal utilities, which describe the relative value of changing from a reference to a non-reference level. The derived marginal utilities were used to calculate relative attribute importance (RAI), where higher values indicated larger effects on preferences. The 95% confidence intervals (CI) were estimated using a bootstrap algorithm over one thousand iterations.
Results
The survey was completed by 170 pts, including 30 from Germany and 30 from Italy. Among pts from Germany and Italy, mean age was 62.9 years and 67% were male. In all, 67% of pts had achieved remission at some point, 70% were diagnosed with AML >6 months before survey completion, and 75% experienced ≥1 relapse event. The estimated MNL models revealed that pts most valued decreasing out-of-pocket cost from $800 to $400 or $200 (RAI = 41.0%, 95% CI 34.5–45.8) and increasing 2-year survival from 30% to 50% or 60% (RAI = 26.7%, 95% CI 21.2–30.5; Figure). Pts preferred therapies with oral administration once daily for 14 or 21 days per month, followed by IV administration 5 days per month, and subcutaneous injection 7 days per month, compared with IV administration in a hospital or clinic 7 days per month (RAI = 14.1%, 95% CI 9.5–20.6). Pt were least concerned about the treatment risks of serious infection, mild-to-moderate stomach problems, and unlike in the global population, time until relapse.
Conclusion
Consistent with findings from the global population, results from this subanalysis of pts from Germany and Italy aged ≥55 years with AML indicated that the most important clinical attribute of MT is improved 2-year survival. Lower out-of-pocket costs and the convenience of an oral pill were also valued. As there is no standard approach to treating AML after intensive chemotherapy, pt preferences should inform decision-making when selecting an MT.
Keyword(s): Acute myeloid leukemia, Elderly, Maintenance, Therapy
Abstract: PB1398
Type: Publication Only
Session title: Acute myeloid leukemia - Clinical
Background
In older patients (pts) with acute myeloid leukemia (AML), intensive chemotherapy can induce complete remission, but responses are often short and overall survival (OS) is poor after relapse. Azacitadine (AZA) maintenance therapies (MT) may improve disease-free survival in pts aged ≥60 years, but have not been shown to improve OS (Oliva EN, et al. ASH 2019; Huls G, et al. Blood 2019). In addition, AZA is given subcutaneously or intravenously (IV), resulting in a high administration burden and potential for infusion reactions. In the phase 3 QUAZAR AML-001 study, a novel oral formulation of AZA was the first MT to show a significant and clinically meaningful improvement in both OS and relapse-free survival (Wei AH, et al. N Engl J Med 2020). While oral AZA offers an effective MT option, little is known about the treatment preferences of pts with AML. We conducted a discrete choice experiment (DCE) survey of pts aged ≥55 years with AML in the USA, Canada, Germany, and Italy to assess the relative importance of key attributes of MT options (Tervonen T, et al. ASH 2020). Globally, pts placed the highest importance on survival probability at 2 years and were willing to accept reduced efficacy for the convenience of oral administration; this subgroup analysis explored the importance that pts in Germany and Italy placed on key factors.
Aims
To examine the relative importance of key attributes of MT among a subgroup of pts aged ≥55 years with AML from Germany and Italy.
Methods
An online DCE was conducted in the USA, Canada, Germany, and Italy between November 2019 and April 2020 to identify preferences for MT attributes among pts aged ≥55 years with AML. DCE data were analyzed using a multinomial logit (MNL) model. The MNL model estimated marginal utilities, which describe the relative value of changing from a reference to a non-reference level. The derived marginal utilities were used to calculate relative attribute importance (RAI), where higher values indicated larger effects on preferences. The 95% confidence intervals (CI) were estimated using a bootstrap algorithm over one thousand iterations.
Results
The survey was completed by 170 pts, including 30 from Germany and 30 from Italy. Among pts from Germany and Italy, mean age was 62.9 years and 67% were male. In all, 67% of pts had achieved remission at some point, 70% were diagnosed with AML >6 months before survey completion, and 75% experienced ≥1 relapse event. The estimated MNL models revealed that pts most valued decreasing out-of-pocket cost from $800 to $400 or $200 (RAI = 41.0%, 95% CI 34.5–45.8) and increasing 2-year survival from 30% to 50% or 60% (RAI = 26.7%, 95% CI 21.2–30.5; Figure). Pts preferred therapies with oral administration once daily for 14 or 21 days per month, followed by IV administration 5 days per month, and subcutaneous injection 7 days per month, compared with IV administration in a hospital or clinic 7 days per month (RAI = 14.1%, 95% CI 9.5–20.6). Pt were least concerned about the treatment risks of serious infection, mild-to-moderate stomach problems, and unlike in the global population, time until relapse.
Conclusion
Consistent with findings from the global population, results from this subanalysis of pts from Germany and Italy aged ≥55 years with AML indicated that the most important clinical attribute of MT is improved 2-year survival. Lower out-of-pocket costs and the convenience of an oral pill were also valued. As there is no standard approach to treating AML after intensive chemotherapy, pt preferences should inform decision-making when selecting an MT.
Keyword(s): Acute myeloid leukemia, Elderly, Maintenance, Therapy