

Contributions
Abstract: PB2368
Type: Publication Only
Background
Health care expenditure in India remains a challenge. Majorly dependent on out of pocket expenditure and private health care, these expenses are now a leading cause of poverty in India and reason to abstain from treatment(1,2). Despite an acknowledged increase in burden of cancers in India, data on the costs of care are lacking. This information is essential for national health care planning and resource allocation. In identifying with this goal we analysed the inpatient hospital care costs for the four most common hematologic cancers from our centre.
Aims
To estimate the inpatient hospital care costs for ALL, AML, NHL and Multiple Myeloma at a tertiary care centre In India.
Methods
Cost data was collected for each hospital inpatient admission beginning July 2015 through January 2018. This was obtained from a prospectively maintained registry which also included baseline demographic information. Hematologic cancers were defined by the WHO classification of tumors of hematopoietic and lymphoid tissues. Inpatient stay was categorized as private room and general ward. The General Ward accommodates five patients in a room with a shared amenities and piped oxygen, suction facility. Private rooms accommodate a single patient and furnished with additional amenities. Patients who were moved to an intensive care unit were not included in this analysis. Standard chemotherapy protocols, antibiotics and antifungal policies with standard of care diagnostic tests were adhered and administered to all patients in an inpatient ward without specialized air handling facilities. The trigger for component transfusion was platelet count of < 10 x 109 /l and Hb < 7 g/dL.
Results
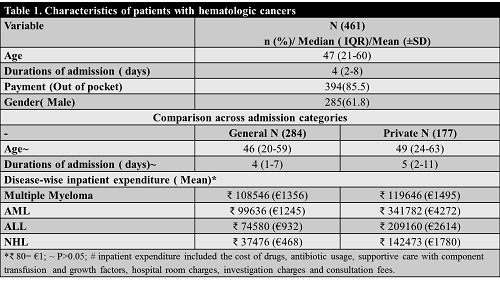
A total of 461 patients were admitted in this period. Characteristics of these patients are detailed in table1. The median distance from home to hospital was 61 km (range: 10–78) and 73(15.8%) patients travelled from another state. Acute Lymphoblastic leukemia was the most frequent diagnosis for admission in 163 (35.4%) patients followed by Non Hodgkin Lymphoma in 144(31.2%). Patients in the private ward were more likely to have availed a health insurance (6.38% vs 2.1%,P <0.01). The median cost of care per inpatient stay was ₹46027.50 (€575) [€ 260 – €1369].
Conclusion
In our analysis, the majority of inpatient hospital expenses are borne out-of-pocket. With a GNI per capita of €1346 and multiple admissions required for chemotherapy administration or complications in hematological cancers; the costs of inpatient care places a high burden on patients. This is despite reduced costs of care when compared globally(3). Variations in treatment protocols across treatment centres in different countries limit the generalization of our findings. However, it is likely that this data is broadly representative of the experience of many tertiary centres within India and also likely to represent many developing countries from where there is limited data. Universal health coverage and better allocation of resources is needed for patients with hematological cancers in India.
Session topic: 36. Quality of life, palliative care, ethics and health economics
Keyword(s): Cancer, Cost analysis
Abstract: PB2368
Type: Publication Only
Background
Health care expenditure in India remains a challenge. Majorly dependent on out of pocket expenditure and private health care, these expenses are now a leading cause of poverty in India and reason to abstain from treatment(1,2). Despite an acknowledged increase in burden of cancers in India, data on the costs of care are lacking. This information is essential for national health care planning and resource allocation. In identifying with this goal we analysed the inpatient hospital care costs for the four most common hematologic cancers from our centre.
Aims
To estimate the inpatient hospital care costs for ALL, AML, NHL and Multiple Myeloma at a tertiary care centre In India.
Methods
Cost data was collected for each hospital inpatient admission beginning July 2015 through January 2018. This was obtained from a prospectively maintained registry which also included baseline demographic information. Hematologic cancers were defined by the WHO classification of tumors of hematopoietic and lymphoid tissues. Inpatient stay was categorized as private room and general ward. The General Ward accommodates five patients in a room with a shared amenities and piped oxygen, suction facility. Private rooms accommodate a single patient and furnished with additional amenities. Patients who were moved to an intensive care unit were not included in this analysis. Standard chemotherapy protocols, antibiotics and antifungal policies with standard of care diagnostic tests were adhered and administered to all patients in an inpatient ward without specialized air handling facilities. The trigger for component transfusion was platelet count of < 10 x 109 /l and Hb < 7 g/dL.
Results
A total of 461 patients were admitted in this period. Characteristics of these patients are detailed in table1. The median distance from home to hospital was 61 km (range: 10–78) and 73(15.8%) patients travelled from another state. Acute Lymphoblastic leukemia was the most frequent diagnosis for admission in 163 (35.4%) patients followed by Non Hodgkin Lymphoma in 144(31.2%). Patients in the private ward were more likely to have availed a health insurance (6.38% vs 2.1%,P <0.01). The median cost of care per inpatient stay was ₹46027.50 (€575) [€ 260 – €1369].
Conclusion
In our analysis, the majority of inpatient hospital expenses are borne out-of-pocket. With a GNI per capita of €1346 and multiple admissions required for chemotherapy administration or complications in hematological cancers; the costs of inpatient care places a high burden on patients. This is despite reduced costs of care when compared globally(3). Variations in treatment protocols across treatment centres in different countries limit the generalization of our findings. However, it is likely that this data is broadly representative of the experience of many tertiary centres within India and also likely to represent many developing countries from where there is limited data. Universal health coverage and better allocation of resources is needed for patients with hematological cancers in India.
Session topic: 36. Quality of life, palliative care, ethics and health economics
Keyword(s): Cancer, Cost analysis