

Contributions
Abstract: PB2374
Type: Publication Only
Background
Diagnostic delay causes unfavourable outcomes among cancer patients. This subject has been widely analysed in solid tumours. However, data regarding haematological malignancies diagnostic delay is scarce worldwide and has never been analysed in Lithuania.
Aims
We aimed to evaluate diagnostic intervals, factors influencing their duration and prolonged time to diagnosis negative effect on clinical outcomes among multiple myeloma and lymphoma patients.
Methods
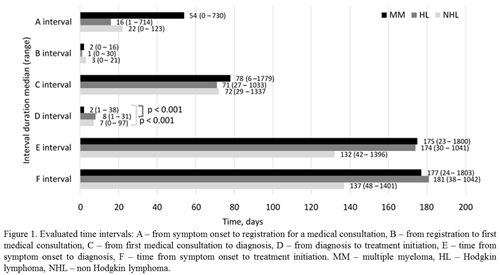
Patients were asked to participate in the study during their scheduled visits in outpatient clinic at a single institution if they had multiple myeloma or lymphoma diagnosis (ICD codes - C90, C81-C84). All participants signed Informed consent form. Following time intervals were evaluated: A - time from symptom onset to registration for a medical consultation, B - from registration to first medical consultation, C - from first medical consultation to diagnosis, D - from diagnosis to treatment initiation, E - from symptom onset to diagnosis, F - time from symptom onset to treatment initiation. Interval durations and majority of influencing factors were assessed based on face-to-face questionnaire. Data of disease characteristics was collected from medical records.
Results
100 patients diagnosed with multiple myeloma (n = 53) and lymphomas (n = 47) were included. Median interval from symptom onset to registration for a medical consultation (A interval) was 30 (0 - 730) days, from registration to consultation (B interval) 2 (0 - 30) days, from first consultation to diagnosis (C interval) 73 (6 - 1779) days, from diagnosis to treatment (D interval) 5 (0 - 97) days. Overall time to diagnosis (E interval) was 151 (23 - 1800) days and did not differ statistically significantly for lymphoma and myeloma patients. Major factors influencing overall diagnostic E interval in multiple linear regression were living in big cities (p = 0.008), anxiety and depression (p = 0.002), self-medication (p = 0.019), more specialists seen before diagnosis (p = 0.022). Longer overall time to diagnosis resulted in higher incidence of multiple myeloma complications (p = 0.024) and more advanced Durie-Salmon stage (p = 0.049) when corrected for age, gender and CIRS comorbidity score. However, longer E interval was not associated with higher ISS stage for myeloma and increased Ann-Arbor stage for lymphomas.
Conclusion
The most important factors causing delay were living in big cities, anxiety and depression, self-medication, more specialists seen before diagnosis. Diagnostic delay may have negative influence on clinical outcomes for multiple myeloma patients. Median time from symptom onset to diagnosis was nearly 5 months indicating that there is space for improvement. Further studies are needed in order to prepare recommendations directed at shortening time to diagnosis and providing clinical benefits for patients with haematological malignancies.
Session topic: 36. Quality of life, palliative care, ethics and health economics
Keyword(s): Diagnosis, lymphoma, Multiple Myeloma
Abstract: PB2374
Type: Publication Only
Background
Diagnostic delay causes unfavourable outcomes among cancer patients. This subject has been widely analysed in solid tumours. However, data regarding haematological malignancies diagnostic delay is scarce worldwide and has never been analysed in Lithuania.
Aims
We aimed to evaluate diagnostic intervals, factors influencing their duration and prolonged time to diagnosis negative effect on clinical outcomes among multiple myeloma and lymphoma patients.
Methods
Patients were asked to participate in the study during their scheduled visits in outpatient clinic at a single institution if they had multiple myeloma or lymphoma diagnosis (ICD codes - C90, C81-C84). All participants signed Informed consent form. Following time intervals were evaluated: A - time from symptom onset to registration for a medical consultation, B - from registration to first medical consultation, C - from first medical consultation to diagnosis, D - from diagnosis to treatment initiation, E - from symptom onset to diagnosis, F - time from symptom onset to treatment initiation. Interval durations and majority of influencing factors were assessed based on face-to-face questionnaire. Data of disease characteristics was collected from medical records.
Results
100 patients diagnosed with multiple myeloma (n = 53) and lymphomas (n = 47) were included. Median interval from symptom onset to registration for a medical consultation (A interval) was 30 (0 - 730) days, from registration to consultation (B interval) 2 (0 - 30) days, from first consultation to diagnosis (C interval) 73 (6 - 1779) days, from diagnosis to treatment (D interval) 5 (0 - 97) days. Overall time to diagnosis (E interval) was 151 (23 - 1800) days and did not differ statistically significantly for lymphoma and myeloma patients. Major factors influencing overall diagnostic E interval in multiple linear regression were living in big cities (p = 0.008), anxiety and depression (p = 0.002), self-medication (p = 0.019), more specialists seen before diagnosis (p = 0.022). Longer overall time to diagnosis resulted in higher incidence of multiple myeloma complications (p = 0.024) and more advanced Durie-Salmon stage (p = 0.049) when corrected for age, gender and CIRS comorbidity score. However, longer E interval was not associated with higher ISS stage for myeloma and increased Ann-Arbor stage for lymphomas.
Conclusion
The most important factors causing delay were living in big cities, anxiety and depression, self-medication, more specialists seen before diagnosis. Diagnostic delay may have negative influence on clinical outcomes for multiple myeloma patients. Median time from symptom onset to diagnosis was nearly 5 months indicating that there is space for improvement. Further studies are needed in order to prepare recommendations directed at shortening time to diagnosis and providing clinical benefits for patients with haematological malignancies.
Session topic: 36. Quality of life, palliative care, ethics and health economics
Keyword(s): Diagnosis, lymphoma, Multiple Myeloma