

Contributions
Abstract: PB2048
Type: Publication Only
Background
Hemophagocytic lymphohistiocytosis (HLH) is a serious, uncommon and underdiagnosed disease, characterized by an exaggerated inflammatory response due to the activation of macrophages and T lymphocytes; and it requires early diagnosis and treatment. HLH can occur as a family/genetic or sporadic/secondary disorder. It can appear spontaneously or triggered by neoplasms, inflammatory disorders or infections, with Epstein Barr virus (EBV) being the most frequent. Clinical manifestations are not specific, presenting these different signs and symptoms, the most common being high temperature, cytopenia and hepatosplenomegaly.
Aims
The aim of the study was to describe the clinical profile of HLH in a tertiary hospital, from 2011 to the present. We analyzed its etiology, clinical and laboratory characteristics, as well as its evolution and treatment.
Methods
Data were collected from patients diagnosed with HLH at the University Hospital of Vigo from October 2011 to the present. Patients who met the diagnostic criteria proposed by the International Hystiocyte Society in 2004 were included, and those treated for HLH who did not meet the criteria previously mentioned were excluded.
Results
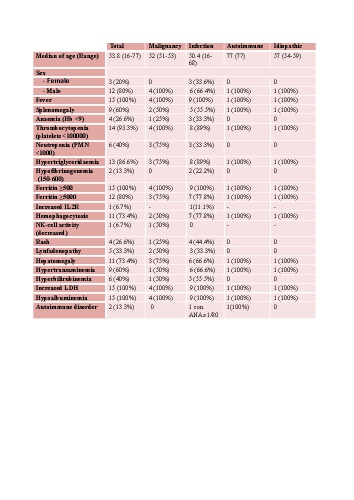
We included 15 cases of HLH, corresponding to 10 patients of which 7 were male and 3 were female, with an overage age of 53.8 years old (range, 16-77 ). 9 cases were secondary to infections, 4 to hematological diseases, 1 to autoimmune disorder and 1 was idiopathic.
All of the patients were attended to with high temperature and high ferritin. Hemophagocytosis was evident in 11 of the 15 cases (in 2 of them a biopsy of the bone marrow was not performed and in 2 others it was inconclusive) . NK-cell activity was studied twice being low in one case. Determination of IL-2R was only carried out in one of the cases being abnormal.
In the majority, high temperature disappeared before 10 days, except in four cases in which it remained 12, 14, 16 and 33 days. 5 of them died: 2 cases were secondary to hematological disease, 2 to infection and 1 secondary to autoimmune disorder.
Among the received treatments we find: HLH-2004 and HLH-1994 Protocols; conventional chemotherapy in cases related to hemopathy, and treatment of causal infection.
Conclusion
In our series, as in the literature, the most frequent cause of secondary HLH is EBV infection; being also the most prevalent diagnostic criteria high temperature and high ferritin.
In most cases a diagnostic delay is observed, since in the initial moment they did not fulfill enough criteria, due in part to the fact that only in some episodes the determination of NK-cell activity and IL-R2 is done, because of the inaccessibility of the studies.
Including HLH in the diagnostic algorithm of persistent febrile syndrome with cytopenias and elevation of acute phase reactants; it would allow an early diagnosis and an early treatment that would improve the prognosis. Likewise, correct etiology and microbiological identification would imply, in our experience, an adaptation of the treatment, avoiding the possible pharmacological toxicity.
Session topic: 31. Infectious diseases, supportive care
Abstract: PB2048
Type: Publication Only
Background
Hemophagocytic lymphohistiocytosis (HLH) is a serious, uncommon and underdiagnosed disease, characterized by an exaggerated inflammatory response due to the activation of macrophages and T lymphocytes; and it requires early diagnosis and treatment. HLH can occur as a family/genetic or sporadic/secondary disorder. It can appear spontaneously or triggered by neoplasms, inflammatory disorders or infections, with Epstein Barr virus (EBV) being the most frequent. Clinical manifestations are not specific, presenting these different signs and symptoms, the most common being high temperature, cytopenia and hepatosplenomegaly.
Aims
The aim of the study was to describe the clinical profile of HLH in a tertiary hospital, from 2011 to the present. We analyzed its etiology, clinical and laboratory characteristics, as well as its evolution and treatment.
Methods
Data were collected from patients diagnosed with HLH at the University Hospital of Vigo from October 2011 to the present. Patients who met the diagnostic criteria proposed by the International Hystiocyte Society in 2004 were included, and those treated for HLH who did not meet the criteria previously mentioned were excluded.
Results
We included 15 cases of HLH, corresponding to 10 patients of which 7 were male and 3 were female, with an overage age of 53.8 years old (range, 16-77 ). 9 cases were secondary to infections, 4 to hematological diseases, 1 to autoimmune disorder and 1 was idiopathic.
All of the patients were attended to with high temperature and high ferritin. Hemophagocytosis was evident in 11 of the 15 cases (in 2 of them a biopsy of the bone marrow was not performed and in 2 others it was inconclusive) . NK-cell activity was studied twice being low in one case. Determination of IL-2R was only carried out in one of the cases being abnormal.
In the majority, high temperature disappeared before 10 days, except in four cases in which it remained 12, 14, 16 and 33 days. 5 of them died: 2 cases were secondary to hematological disease, 2 to infection and 1 secondary to autoimmune disorder.
Among the received treatments we find: HLH-2004 and HLH-1994 Protocols; conventional chemotherapy in cases related to hemopathy, and treatment of causal infection.
Conclusion
In our series, as in the literature, the most frequent cause of secondary HLH is EBV infection; being also the most prevalent diagnostic criteria high temperature and high ferritin.
In most cases a diagnostic delay is observed, since in the initial moment they did not fulfill enough criteria, due in part to the fact that only in some episodes the determination of NK-cell activity and IL-R2 is done, because of the inaccessibility of the studies.
Including HLH in the diagnostic algorithm of persistent febrile syndrome with cytopenias and elevation of acute phase reactants; it would allow an early diagnosis and an early treatment that would improve the prognosis. Likewise, correct etiology and microbiological identification would imply, in our experience, an adaptation of the treatment, avoiding the possible pharmacological toxicity.
Session topic: 31. Infectious diseases, supportive care