

Contributions
Abstract: PB2459
Type: Publication Only
Background
Nutritional status is significantly compromised during the hematopoietic stem cell transplantation (HSCT), which not only postpones the period of engraftment but also plays a role in graft versus host disease (GVHD), veno-occlusive disease (VOD) and hospitalization in the ICU. Moreover, given conditioning regimen composed of high-dose chemotherapy or total body irradiation (TBI) triggering various side effects that disturb nutritional intake, such as stomatitis, nausea, vomiting, loss of appetite and diarrhea, it’s a challenging task to maintain healthy nutritional status. However, less literature is available regarding nutrition status compromise (average amount and duration of inadequate intake of nutrients) in patients undergoing HSCT which hampers with planning during HSCT. The need for similar data is even more pertinent in developing countries where the average nutritional status of the citizen is poor.
Aims
To assess and compare Estimated Energy Requirement, dietary intake and weight changes from the day of the start of conditioning regimen to 14 days after transplantation or discharge.
Methods
This prospective observational study carried out in the Department of Internal Medicine in association with department of Dietetics PGIMER, Chandigarh. A total of 20 patients (12 auto and 8 allo) undergoing HSCT were included between 2016-2017. Body mass index (BMI) and Mid upper arm circumference (MUAC) was measured daily, and recording of all foods and fluid taken by patients was done using diet chart performa. Based on daily food consumption Calorie, protein, carbohydrate, and fat intake were calculated.
The Estimated Energy Requirement ( EER) for Maintenance is the dietary energy intake that is predicted to maintain energy balance in healthy individuals or groups of individuals at current levels of body size and level of physical activity. EER was calculated for each patient according to their physical activity level, based on dietary reference intakes (DRI) equations and was compared with actual calorie intake.
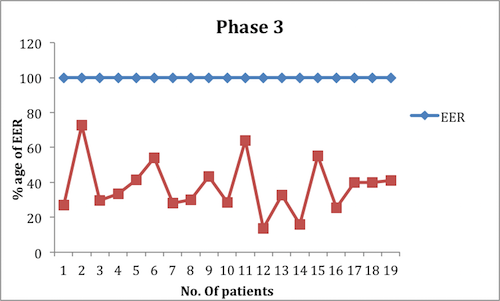
The Transplantation period was divided into four phases; phase 1(start of conditioning to D-1), phase 2 (D0 to D+7), phase 3(iD+8 to D+14) and phase 4 (at the time of discharge).
Results
The median age was 45.5 years (Range 10-64). The average calories, carbohydrates, protein, and fats intake by all patients undergoing HSCT had decreasing trend during all phases except for the time of discharge. There was a significant effect of duration on weight (p=0.002), BMI (p=0.000), calorie intake (p=0.002) and fats intake during different phases (p <=0.001). There was no significant effect of duration on protein (p = 0.128) and carbohydrates intake (p = 0.051).
None (0%) of the patients met 100% of EER in any phase of transplant duration. Two (10%) at phase 1, eight (40%) at phase 2, 15 (75%) at phase 3 and three (15%) at discharge did not meet even 50% of EER (image).
Conclusion
There is a significant compromise in nutrients intake in patients undergoing HSCT. The nutritional status continues to worsen unless patient recovers fully and is fit for discharge. Therefore, there is a need to step up our effort to supplement nutrition by giving oral and parenteral supplements. Further study can be done in HSCT patients not meeting EER, analyzing the effect on engraftment, GVHD, VOD and hospitalization stay.
Session topic: 23. Stem cell transplantation - Clinical
Keyword(s): Hematopoietic cell transplantation
Abstract: PB2459
Type: Publication Only
Background
Nutritional status is significantly compromised during the hematopoietic stem cell transplantation (HSCT), which not only postpones the period of engraftment but also plays a role in graft versus host disease (GVHD), veno-occlusive disease (VOD) and hospitalization in the ICU. Moreover, given conditioning regimen composed of high-dose chemotherapy or total body irradiation (TBI) triggering various side effects that disturb nutritional intake, such as stomatitis, nausea, vomiting, loss of appetite and diarrhea, it’s a challenging task to maintain healthy nutritional status. However, less literature is available regarding nutrition status compromise (average amount and duration of inadequate intake of nutrients) in patients undergoing HSCT which hampers with planning during HSCT. The need for similar data is even more pertinent in developing countries where the average nutritional status of the citizen is poor.
Aims
To assess and compare Estimated Energy Requirement, dietary intake and weight changes from the day of the start of conditioning regimen to 14 days after transplantation or discharge.
Methods
This prospective observational study carried out in the Department of Internal Medicine in association with department of Dietetics PGIMER, Chandigarh. A total of 20 patients (12 auto and 8 allo) undergoing HSCT were included between 2016-2017. Body mass index (BMI) and Mid upper arm circumference (MUAC) was measured daily, and recording of all foods and fluid taken by patients was done using diet chart performa. Based on daily food consumption Calorie, protein, carbohydrate, and fat intake were calculated.
The Estimated Energy Requirement ( EER) for Maintenance is the dietary energy intake that is predicted to maintain energy balance in healthy individuals or groups of individuals at current levels of body size and level of physical activity. EER was calculated for each patient according to their physical activity level, based on dietary reference intakes (DRI) equations and was compared with actual calorie intake.
The Transplantation period was divided into four phases; phase 1(start of conditioning to D-1), phase 2 (D0 to D+7), phase 3(iD+8 to D+14) and phase 4 (at the time of discharge).
Results
The median age was 45.5 years (Range 10-64). The average calories, carbohydrates, protein, and fats intake by all patients undergoing HSCT had decreasing trend during all phases except for the time of discharge. There was a significant effect of duration on weight (p=0.002), BMI (p=0.000), calorie intake (p=0.002) and fats intake during different phases (p <=0.001). There was no significant effect of duration on protein (p = 0.128) and carbohydrates intake (p = 0.051).
None (0%) of the patients met 100% of EER in any phase of transplant duration. Two (10%) at phase 1, eight (40%) at phase 2, 15 (75%) at phase 3 and three (15%) at discharge did not meet even 50% of EER (image).
Conclusion
There is a significant compromise in nutrients intake in patients undergoing HSCT. The nutritional status continues to worsen unless patient recovers fully and is fit for discharge. Therefore, there is a need to step up our effort to supplement nutrition by giving oral and parenteral supplements. Further study can be done in HSCT patients not meeting EER, analyzing the effect on engraftment, GVHD, VOD and hospitalization stay.
Session topic: 23. Stem cell transplantation - Clinical
Keyword(s): Hematopoietic cell transplantation