

Contributions
Abstract: PB2179
Type: Publication Only
Background
"Thrombosis is often reported in cancer"Trousseau wrote in 1865.Multiple myeloma(MM)is associated with venous-thromboembolism.Moreover bleeding-complications are possible in plasma-cell-disorders and are cause of early mortality.Data available in this setting are rare.
Aims
We’d like to share our experience regarding 138 patients with these events retrospectively analysed.
Methods
We reviewed 20 bleeding and 118 thrombotic events consecutively diagnosed and managed between 1999 to 2018 in the median-time of 18 years, median follow up 12,5 years(10,2-19).
Results
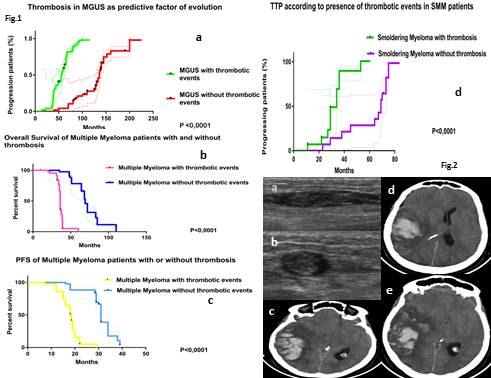
We reported 4 bleeding events in amyloidosis patients:3 periorbital hemorrhages related to X-factor-deficiency and one intestinal-bleeding.We described 15 hemorragic events in MM patients under treatment:one of them was lifethreatening(an extensive brain hemorrhage)and 4 gastrointestinal-bleeding.11 events were minor mucocutaneous-haemorrhages.Among risk-factors we have high monoclonal-component at diagnosis(13).A 49-year old female died during induction-therapy of a fatal brain hemorrhage.On CT an extended intracranial hemorrhage developed in right parietal region(Fig.2c-e).Platelet and coagulation-exams were normal.Hypothesized mechanisms are an acquired platelet disfunction o an amyloidotic deposition of fibrils.We had 5 events after osteomedullary-biopsies:we recommend a good post-procedure-compression.Within thrombotic manifestations we have 69-events in MGUS(59 venous,10 arterial),29 events in MM(22 venous,7 arterial)and 20 events in SMM patients(18 venous,2 arterial).Thrombophilic screening was negative.Venous thromboses described were at diagnosis not at relapse(75/99).We had one case of massive lethal pulmonary embolism.We have described 7 thrombotic manifestations in MM-patients at the time of diagnosis before the start of therapy,highlighting how the disease is associated with a thrombogenic condition.Among risk factors of disease we have ISS score(III 39, II 7 and I 3),elevated serum-FLC(40/49).Therapy-consisted-of dexamethasone(29),chemotherapy(9),lenalidomide(8),KRD(2),doxorubicin(3),thalidomide(5),pomalidomide(2 patients).We chose low molecular heparin for prophylaxis.Among MGUS patients 48 evolved with median TTP of 56 months(14-90).We compared TTP with an homogeneous group of 48 patients(69 months,51-110)matched by age and risk-profile,with evidence of a shorter progression-time in patients with MGUS and thrombosis(Fig1a,Longrank-test-95%IC 2,9-9,HR5).M-protein level is a risk factor.Moreover in our study 14 SMM-patients evolved with medium time of 34 months(11-53).We have compared TTP with an age and risk-profile-matched-SMM-patients-group(14-patients),median-time-69-months,range-29-75(Fig1d).L-Rtest,95%CI,HR3,4),showing a shorter time for SMM-series with thrombosis.Crosstalk between microenvironment and clone can facilitate progression.Finally we compared OS and PFS among our 44 MM patients under therapy and thrombosis and a similar group regarding age and ISS score,demonstrating how outcome and PFS are worse in patients with thrombosis(Fig 1b-c).For first series median OS is of 36 months(20-60)and PFS of 18,5 months(range 7-29)and for second-series without thrombosis median OS of 69 months(35-110)and PFS of 31 months(6-39),L-R test,95%CI,HR 4,7 for OS and HR4,2 PFS).
Conclusion
Our study is limited:heterogeneity of population and no information about cytogenetics.Cancer protrombogenicity may promote angiogenesis,metastasis and poorer prognosis.Prospective studies are needed to verify our conclusions and to investigate exact pathogenesis.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Thrombophilia, Bleeding, Multiple Myeloma, Outcome
Abstract: PB2179
Type: Publication Only
Background
"Thrombosis is often reported in cancer"Trousseau wrote in 1865.Multiple myeloma(MM)is associated with venous-thromboembolism.Moreover bleeding-complications are possible in plasma-cell-disorders and are cause of early mortality.Data available in this setting are rare.
Aims
We’d like to share our experience regarding 138 patients with these events retrospectively analysed.
Methods
We reviewed 20 bleeding and 118 thrombotic events consecutively diagnosed and managed between 1999 to 2018 in the median-time of 18 years, median follow up 12,5 years(10,2-19).
Results
We reported 4 bleeding events in amyloidosis patients:3 periorbital hemorrhages related to X-factor-deficiency and one intestinal-bleeding.We described 15 hemorragic events in MM patients under treatment:one of them was lifethreatening(an extensive brain hemorrhage)and 4 gastrointestinal-bleeding.11 events were minor mucocutaneous-haemorrhages.Among risk-factors we have high monoclonal-component at diagnosis(13).A 49-year old female died during induction-therapy of a fatal brain hemorrhage.On CT an extended intracranial hemorrhage developed in right parietal region(Fig.2c-e).Platelet and coagulation-exams were normal.Hypothesized mechanisms are an acquired platelet disfunction o an amyloidotic deposition of fibrils.We had 5 events after osteomedullary-biopsies:we recommend a good post-procedure-compression.Within thrombotic manifestations we have 69-events in MGUS(59 venous,10 arterial),29 events in MM(22 venous,7 arterial)and 20 events in SMM patients(18 venous,2 arterial).Thrombophilic screening was negative.Venous thromboses described were at diagnosis not at relapse(75/99).We had one case of massive lethal pulmonary embolism.We have described 7 thrombotic manifestations in MM-patients at the time of diagnosis before the start of therapy,highlighting how the disease is associated with a thrombogenic condition.Among risk factors of disease we have ISS score(III 39, II 7 and I 3),elevated serum-FLC(40/49).Therapy-consisted-of dexamethasone(29),chemotherapy(9),lenalidomide(8),KRD(2),doxorubicin(3),thalidomide(5),pomalidomide(2 patients).We chose low molecular heparin for prophylaxis.Among MGUS patients 48 evolved with median TTP of 56 months(14-90).We compared TTP with an homogeneous group of 48 patients(69 months,51-110)matched by age and risk-profile,with evidence of a shorter progression-time in patients with MGUS and thrombosis(Fig1a,Longrank-test-95%IC 2,9-9,HR5).M-protein level is a risk factor.Moreover in our study 14 SMM-patients evolved with medium time of 34 months(11-53).We have compared TTP with an age and risk-profile-matched-SMM-patients-group(14-patients),median-time-69-months,range-29-75(Fig1d).L-Rtest,95%CI,HR3,4),showing a shorter time for SMM-series with thrombosis.Crosstalk between microenvironment and clone can facilitate progression.Finally we compared OS and PFS among our 44 MM patients under therapy and thrombosis and a similar group regarding age and ISS score,demonstrating how outcome and PFS are worse in patients with thrombosis(Fig 1b-c).For first series median OS is of 36 months(20-60)and PFS of 18,5 months(range 7-29)and for second-series without thrombosis median OS of 69 months(35-110)and PFS of 31 months(6-39),L-R test,95%CI,HR 4,7 for OS and HR4,2 PFS).
Conclusion
Our study is limited:heterogeneity of population and no information about cytogenetics.Cancer protrombogenicity may promote angiogenesis,metastasis and poorer prognosis.Prospective studies are needed to verify our conclusions and to investigate exact pathogenesis.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Thrombophilia, Bleeding, Multiple Myeloma, Outcome