

Contributions
Abstract: PB2235
Type: Publication Only
Background
Overall survival in Multiple Myeloma (MM) improved in last decades with the introduction of newer agents and broader use of autologous hematopoietic stem cell transplantation. Besides this, early mortality (EM) is still a concern in newly diagnosed MM. Data for EM comes from large prospective trials of selected MM populations and different time cut-off points are used in different studies.
Aims
To evaluate most common causes of EM in MM, risk factors for EM and to flash on do’s and don’ts in high risk cases.
Methods
Retrospective data from 37 newly diagnosed MM patients between 01.01.2003-30.10.2017 and died within 12 months of diagnosis and as control group 52 newly diagnosed MM patients who lived longer than 12 months were analyzed. Four different cut-off time points for early mortality was defined as 1 month (EM1), 3 months (EM3), 6 months (EM6) and 12 months (EM12). Univariate analyses were done by Chi-square test for categorical and by t-test for numerical variables, respectively. Multivariate analyses were done by Cox regression analysis.
Results
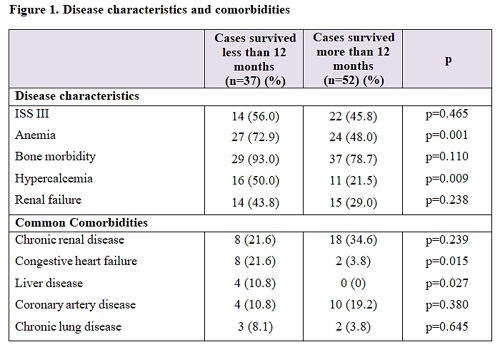
Median age was 59 (range, 45-82 years) and was not different from cases lived longer than 12 months (p=0,822). Males and females were 56.8 % and 43.2 % respectively. Disease characteristics and comorbidities are summarized in Figure 1. Most common cause of mortality was acute renal injury (86.5%). Median survival was 3.8 months for EM12. Multivariate analysis showed anemia (HR: 4.20, p: 0.003), and hypercalcemia (HR: 2.44, p: 0.012) as independent risk factors for EM12; anemia (HR: 3.79, p: 0,015) and hypercalcemia (HR: 2.39, p: 0.029) for EM6, anemia (HR: 4.69, p: 0.041) for EM3. Renal failure was also more frequent in EM12 (p=0,200). Congestive heart failure was associated with increased mortality in EM12 (HR: 3.10, p: 0.005) and EM6 (HR: 3.46, p: 0.005). Bortezomib based induction regimens were less frequently associated with mortality in EM12 (HR: 0.23, p<0.001), EM6 (HR: 0.22, p: 0,003) and EM3 (HR: 0.14, p: 0.01) in multivariate analysis. Types of paraprotein, extramedullary disease, adjusted Charlson Comorbidity Score were not statistically different between early mortality groups at any cut-off point of survival times. Response to induction regimen was not included in analysis due to missing data.
Conclusion
Our study was first to detect anemia as a risk factor for EM in MM. Congestive heart failure was a risk factor as a comorbidity. Renal failure was also a risk factor for EM although not significant but there are studies showing renal failure as a risk factor for EM. These high risk patients should be treated with newer, less toxic agents.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Anemia, bortezomib, Mortality, Multiple Myeloma
Abstract: PB2235
Type: Publication Only
Background
Overall survival in Multiple Myeloma (MM) improved in last decades with the introduction of newer agents and broader use of autologous hematopoietic stem cell transplantation. Besides this, early mortality (EM) is still a concern in newly diagnosed MM. Data for EM comes from large prospective trials of selected MM populations and different time cut-off points are used in different studies.
Aims
To evaluate most common causes of EM in MM, risk factors for EM and to flash on do’s and don’ts in high risk cases.
Methods
Retrospective data from 37 newly diagnosed MM patients between 01.01.2003-30.10.2017 and died within 12 months of diagnosis and as control group 52 newly diagnosed MM patients who lived longer than 12 months were analyzed. Four different cut-off time points for early mortality was defined as 1 month (EM1), 3 months (EM3), 6 months (EM6) and 12 months (EM12). Univariate analyses were done by Chi-square test for categorical and by t-test for numerical variables, respectively. Multivariate analyses were done by Cox regression analysis.
Results
Median age was 59 (range, 45-82 years) and was not different from cases lived longer than 12 months (p=0,822). Males and females were 56.8 % and 43.2 % respectively. Disease characteristics and comorbidities are summarized in Figure 1. Most common cause of mortality was acute renal injury (86.5%). Median survival was 3.8 months for EM12. Multivariate analysis showed anemia (HR: 4.20, p: 0.003), and hypercalcemia (HR: 2.44, p: 0.012) as independent risk factors for EM12; anemia (HR: 3.79, p: 0,015) and hypercalcemia (HR: 2.39, p: 0.029) for EM6, anemia (HR: 4.69, p: 0.041) for EM3. Renal failure was also more frequent in EM12 (p=0,200). Congestive heart failure was associated with increased mortality in EM12 (HR: 3.10, p: 0.005) and EM6 (HR: 3.46, p: 0.005). Bortezomib based induction regimens were less frequently associated with mortality in EM12 (HR: 0.23, p<0.001), EM6 (HR: 0.22, p: 0,003) and EM3 (HR: 0.14, p: 0.01) in multivariate analysis. Types of paraprotein, extramedullary disease, adjusted Charlson Comorbidity Score were not statistically different between early mortality groups at any cut-off point of survival times. Response to induction regimen was not included in analysis due to missing data.
Conclusion
Our study was first to detect anemia as a risk factor for EM in MM. Congestive heart failure was a risk factor as a comorbidity. Renal failure was also a risk factor for EM although not significant but there are studies showing renal failure as a risk factor for EM. These high risk patients should be treated with newer, less toxic agents.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Anemia, bortezomib, Mortality, Multiple Myeloma