

Contributions
Abstract: PB2229
Type: Publication Only
Background
Amyloidosis is a rare disease characterized by tissue deposition of insoluble fibrils created by the aggregation of misfolded proteins. Cardiac involvement is common and associated with an increased risk of morbidity and mortality. The most frequent types of amyloidosis are light-chain (AL) and mutant or wild-type transthyretin (TTR). AL amyloidosis caused by the deposition of misfolded kappa or lambda light chains in patients with an underlying plasma cell malignancy. Differential diagnosis between AL and TTR cardiac amyloidosis is mandatory because prognosis and therapy are different, but it is not always easy as non-invasive techniques are not specific.
Aims
We report three patients with a monoclonal gammopathy and wild-type TTR amyloidosis
Methods
Case reports
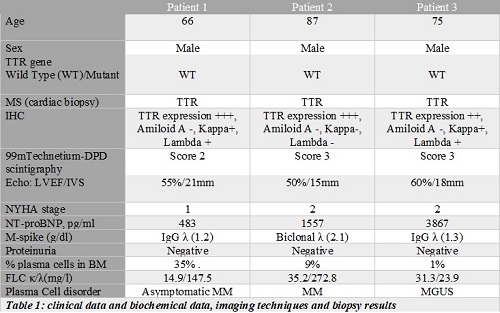
Patient 1. A 66-year old men was sent for haematological evaluation after an ischemic stroke. He was otherwise asymptomatic. An echocardiogram showed a concentric left ventricular hypertrophy suggesting cardiac amyloidosis. Blood tests showed normal counts, a monoclonal component and an increase in free light chains (FLC). A cardiac biopsy showed Congo Red positive deposits. Immunohystochemistry (IHC) was not diagnostic. Mass spectrometry (MS) confirmed the diagnosis of TTR amyloidosis. Fifty months from diagnosis, he remains asymptomatic with stable FLC and NT-proBNP.
Patient 2. A 87 year old men was admitted to our Hospital with a two-month history of cough, edemas, and dyspnea. He had anemia, thrombopenia, a biclonal component and an increase in FLC. A cardiac biopsy with IHC and MS confirmed the diagnosis of TTR amyloidosis. He was begun on cyclophosphamide, prednisone and thalidomide with improvement of the blood counts and decrease of the M-spike. Thirteen months from diagnosis, he remains alive with cardiological support.
Patient 3. A 75-year-old male was evaluated at our centre with a three-month history of edemas and shortness of breath. A diagnosis of monoclonal gammopathy of unknown significance (MGUS) had been made elsewhere nine years before. Echocardiography showed a severe concentric left ventricular hypertrophy. A cardiac biopsy with IHC and MS confirmed the diagnosis of TTR amyloidosis. Ten months from diagnosis he remains stable with diuretic therapy. MGUS remains also stable.
Results
Our three patients are elderly males with a MGUS and a positive SC. Although IHC studies showed TTR deposition in the heart, a faint positive staining with anti-TTR can be seen in AL specimens. In the three cases, MS confirmed the presence of TTR and ruled out deposition of light chains.
Conclusion
Most cardiac amyloidosis are either due to TTR or light chain deposition. AL cardiac amyloidosis has a worse prognosis and the underlying neoplastic clone can be treated with anti-myeloma drugs. Differential diagnosis between AL and TTR amyloidosis may be complicated. Firstly, wild-type TTR amyloidosis may be more prevalent among elderly patients than previously thought. Secondly, many elderly patients have monoclonal gammopathies so the presence of a MGUS does not mean that amyloidosis is AL. Echocardiography or MRI of the heart cannot differentiate between the two types. Scintigraphy (SC) with 99Tc is always positive in patients with cardiac TTR-amyloidosis but up to 10% of AL cases may show a positive score. Immuno-electronic microscopy is not available in most centres.
Differential diagnosis between cardiac AL and TTR amyloidosis is mandatory because subtyping of the amyloid has significant implications in the management of patients and prognosis. MS might be essential.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Amyloidosis, Monoclonal gammopathy
Abstract: PB2229
Type: Publication Only
Background
Amyloidosis is a rare disease characterized by tissue deposition of insoluble fibrils created by the aggregation of misfolded proteins. Cardiac involvement is common and associated with an increased risk of morbidity and mortality. The most frequent types of amyloidosis are light-chain (AL) and mutant or wild-type transthyretin (TTR). AL amyloidosis caused by the deposition of misfolded kappa or lambda light chains in patients with an underlying plasma cell malignancy. Differential diagnosis between AL and TTR cardiac amyloidosis is mandatory because prognosis and therapy are different, but it is not always easy as non-invasive techniques are not specific.
Aims
We report three patients with a monoclonal gammopathy and wild-type TTR amyloidosis
Methods
Case reports
Patient 1. A 66-year old men was sent for haematological evaluation after an ischemic stroke. He was otherwise asymptomatic. An echocardiogram showed a concentric left ventricular hypertrophy suggesting cardiac amyloidosis. Blood tests showed normal counts, a monoclonal component and an increase in free light chains (FLC). A cardiac biopsy showed Congo Red positive deposits. Immunohystochemistry (IHC) was not diagnostic. Mass spectrometry (MS) confirmed the diagnosis of TTR amyloidosis. Fifty months from diagnosis, he remains asymptomatic with stable FLC and NT-proBNP.
Patient 2. A 87 year old men was admitted to our Hospital with a two-month history of cough, edemas, and dyspnea. He had anemia, thrombopenia, a biclonal component and an increase in FLC. A cardiac biopsy with IHC and MS confirmed the diagnosis of TTR amyloidosis. He was begun on cyclophosphamide, prednisone and thalidomide with improvement of the blood counts and decrease of the M-spike. Thirteen months from diagnosis, he remains alive with cardiological support.
Patient 3. A 75-year-old male was evaluated at our centre with a three-month history of edemas and shortness of breath. A diagnosis of monoclonal gammopathy of unknown significance (MGUS) had been made elsewhere nine years before. Echocardiography showed a severe concentric left ventricular hypertrophy. A cardiac biopsy with IHC and MS confirmed the diagnosis of TTR amyloidosis. Ten months from diagnosis he remains stable with diuretic therapy. MGUS remains also stable.
Results
Our three patients are elderly males with a MGUS and a positive SC. Although IHC studies showed TTR deposition in the heart, a faint positive staining with anti-TTR can be seen in AL specimens. In the three cases, MS confirmed the presence of TTR and ruled out deposition of light chains.
Conclusion
Most cardiac amyloidosis are either due to TTR or light chain deposition. AL cardiac amyloidosis has a worse prognosis and the underlying neoplastic clone can be treated with anti-myeloma drugs. Differential diagnosis between AL and TTR amyloidosis may be complicated. Firstly, wild-type TTR amyloidosis may be more prevalent among elderly patients than previously thought. Secondly, many elderly patients have monoclonal gammopathies so the presence of a MGUS does not mean that amyloidosis is AL. Echocardiography or MRI of the heart cannot differentiate between the two types. Scintigraphy (SC) with 99Tc is always positive in patients with cardiac TTR-amyloidosis but up to 10% of AL cases may show a positive score. Immuno-electronic microscopy is not available in most centres.
Differential diagnosis between cardiac AL and TTR amyloidosis is mandatory because subtyping of the amyloid has significant implications in the management of patients and prognosis. MS might be essential.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Amyloidosis, Monoclonal gammopathy