

Contributions
Abstract: PB1732
Type: Publication Only
Background
outcome of AML patients (pts) older than 60 years is poor because of unfavourable disease characteristics and of comorbidities, frequently tailoring under-powered treatment. The complete remission (CR) rate after intensive treatments is lower than in younger pts, with relapse incidence and mortality associated to treatment (TRM) being higher. Rarely, elderly pts who relapse after initial remission receive salvage treatments aiming to obtain further disease remission.
Aims
to evaluate the feasibility and efficacy of intensive treatments in our elderly pts with relapsed AML.
Methods
retrospective analysis of data from 50 pts with AML in CR relapsed between 2/2002-1/2018. Criteria for pts selection to receive salvage treatments: PS (ECOG) ≤ 2, renal and hepatic parameters within normal ranges or < 2 times normal values, no active infections and cardiac ejection fraction > 50%.
Results
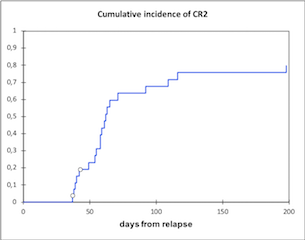
median pts age at relapse was 70 (61-81). Cytogenetics and molecular data at relapse were available only for a minority of pts and were not analyzed. Median time to relapse was 227 days (range 42-3369). Overall, 30 pts (60%) received at least one reinduction treatment: chemotherapy (CHT) in 23 cases, upfront allogeneic transplantation (alloSCT) in 3 cases, alloSCT after no response to CHT in 4 cases. Eleven pts had previously received an autologous SCT, 19 pts CHT with intermediate or high dose cytarabine, as consolidation of first CR. Twenty-one pts (68%) obtained second CR (CR2), 15 after CHT alone, 3 after upfront alloSCT, 3 after CHT and alloSCT. TRM was 27% (8 pts), overall, 17% after CHT alone, 75% after upfront alloSCT, 50% after CHT and alloSCT. Of the 15 pts in CR2 after CHT alone, 10 did not receive further treatments, 5 received an alloSCT. At last follow up 4 pts out of 30 (13%) are alive in CR2, with a median survival from relapse of 421 days (255-4906). Median OS from relapse of all pts who received any reinduction treatment was 276 days (33-4904). Median OS from relapse of pts who obtained the CR2 750 days (137-4904). Median DFS from CR2 was 429 days (29-4848).
Conclusion
intensive reinduction approaches proved feasible in our elderly pts with relapsed AML. The CR rate was similar to that obtained at diagnosis. Actually, TRM was high, in particular after alloSCT (57% overall). Of note, 4 pts (57%) had active disease at time of alloSCT. Moreover, median age of the treated population was high. Anyway, several pts obtained prolonged overall and disease free survival. We conclude that elderly pts with relapsed AML, fit according to PS and general criteria, could benefit from an intensive curative approach. Recent introduction of new strategies to prevent and treat potentially fatal complications after alloSCT, in particular infections and graft versus host disease, should prospectively reduce TRM and improve survival.
Session topic: 4. Acute myeloid leukemia - Clinical
Keyword(s): AML, Elderly, Treatment
Abstract: PB1732
Type: Publication Only
Background
outcome of AML patients (pts) older than 60 years is poor because of unfavourable disease characteristics and of comorbidities, frequently tailoring under-powered treatment. The complete remission (CR) rate after intensive treatments is lower than in younger pts, with relapse incidence and mortality associated to treatment (TRM) being higher. Rarely, elderly pts who relapse after initial remission receive salvage treatments aiming to obtain further disease remission.
Aims
to evaluate the feasibility and efficacy of intensive treatments in our elderly pts with relapsed AML.
Methods
retrospective analysis of data from 50 pts with AML in CR relapsed between 2/2002-1/2018. Criteria for pts selection to receive salvage treatments: PS (ECOG) ≤ 2, renal and hepatic parameters within normal ranges or < 2 times normal values, no active infections and cardiac ejection fraction > 50%.
Results
median pts age at relapse was 70 (61-81). Cytogenetics and molecular data at relapse were available only for a minority of pts and were not analyzed. Median time to relapse was 227 days (range 42-3369). Overall, 30 pts (60%) received at least one reinduction treatment: chemotherapy (CHT) in 23 cases, upfront allogeneic transplantation (alloSCT) in 3 cases, alloSCT after no response to CHT in 4 cases. Eleven pts had previously received an autologous SCT, 19 pts CHT with intermediate or high dose cytarabine, as consolidation of first CR. Twenty-one pts (68%) obtained second CR (CR2), 15 after CHT alone, 3 after upfront alloSCT, 3 after CHT and alloSCT. TRM was 27% (8 pts), overall, 17% after CHT alone, 75% after upfront alloSCT, 50% after CHT and alloSCT. Of the 15 pts in CR2 after CHT alone, 10 did not receive further treatments, 5 received an alloSCT. At last follow up 4 pts out of 30 (13%) are alive in CR2, with a median survival from relapse of 421 days (255-4906). Median OS from relapse of all pts who received any reinduction treatment was 276 days (33-4904). Median OS from relapse of pts who obtained the CR2 750 days (137-4904). Median DFS from CR2 was 429 days (29-4848).
Conclusion
intensive reinduction approaches proved feasible in our elderly pts with relapsed AML. The CR rate was similar to that obtained at diagnosis. Actually, TRM was high, in particular after alloSCT (57% overall). Of note, 4 pts (57%) had active disease at time of alloSCT. Moreover, median age of the treated population was high. Anyway, several pts obtained prolonged overall and disease free survival. We conclude that elderly pts with relapsed AML, fit according to PS and general criteria, could benefit from an intensive curative approach. Recent introduction of new strategies to prevent and treat potentially fatal complications after alloSCT, in particular infections and graft versus host disease, should prospectively reduce TRM and improve survival.
Session topic: 4. Acute myeloid leukemia - Clinical
Keyword(s): AML, Elderly, Treatment