

Contributions
Abstract: PB2279
Type: Publication Only
Background
Langerhans cell histiyocytosis (LCH) is a rare disease of histiocytes that is more prevalent in childhood. The etiology is unknown. Any organ or system may be affected in LCH. Bones, skin, and pituitary gland are frequently involved. Clinical presentation may be diverse according to the organ affected. Treatment modality depends on the extent of the disease. With mild symptoms and no risk organ involvement methotraxate, azathiopurin, thalidomide can be used or patient can be carefully observed without therapy. Symptomatic and mutisystemic LCH with or without risk organ involvement require chemotherapy.
Aims
Our aim is to evaluate clinical characteristics and outcome of adult onset LCH patients in our instutition.
Methods
We retrospectively evaluated adult patients diagnosed as LCH at Ege University Hospital between 2000-2017. All patients were screened by total bone X-ray survey and/or bone scintigraphy, abdominal and chest computerized tomography , cranial magnetic resonance imaging and some of the patients by positron emission tomography. Bone marrow aspiration and biopsy were performed in all patients in order to evaluate the possible bone marrow infiltration. Complete blood count, blood chemistry, erythrocyte sedimentation rate, coagulation studies, thyroid stimulating hormone and free T4, other pituitary gland hormones if pituitary gland is involved, and urine strip test were analyzed. Patients were stratified according to extent of the disease:Single system LCH (SS-LCH): One organ or system involved. It may be uni- or multifocal,Multisystem LCH (MS-LCH): Two or more organs/systems involved.Choice of treatment, dose and duration of drugs, radiotherapy fields and dosage, side effects of the treatment modalities were recorded. Outcome of the patients were evaluated.
Results
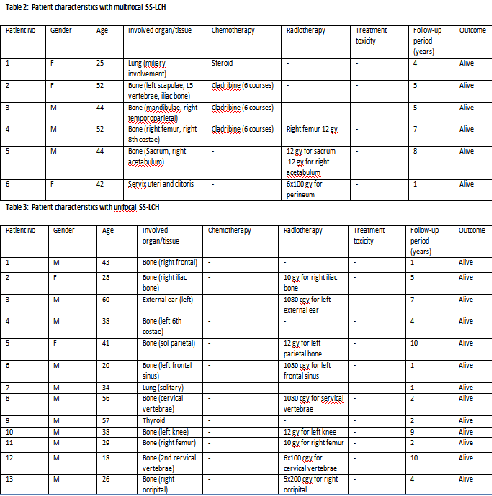
A total of 27 patients were diagnosed and treated in our hospital. Mean age at diagnosis was 38.3 years, 19 of them were male. There were 8 patients with MS-LCH, 13 with unifocal SS-LCH, and 6 with multifocal SS-LCH. Patients' characteristics were summarized in the tables 1, 2 and 3. All of our patients are alive. There was only one treatment toxicity, diabetes insipidus, in a patient with pons and mastoid lesion after radiotherapy. Most of MS-LCH and multifocal SS-LCH patients received systemic treatment, whereas unifocal SS-LCH.
Table 1: Patient characteristics with MS-LCH
Patient No | Gender | Age | Involved organ/tissue | Chemotherapy | Radiotherapy | Treatment toxicity | Follow-up period (years) | Outcome |
1 | M | 36 | Lung,Skin | Cladribine (6 courses) | - | - | 4 | Alive |
2 | M | 40 | Thyroid,Gum | Chemotherapy for concomitant thyroidpapillary carcinoma | - | - | 3 | Alive |
3 | M | 32 | Skin,Gum | Cladribine (6 courses) | - | - | 12 | Alive |
4 | M | 38 | Bone (parietal),Lung | Cladribine (5 courses) | - | - | 1 | Alive |
5 | F | 47 | Bone (left mandible, left tibia),Pons,Lung | - | Pons-mastoid 10x2 gy,tibia 10x2 gy | Diabetes insipidus | 8 | Alive |
6 | F | 47 | Bone (left parietal, left femur),Skin | Cladribine (6 courses) | - | - | 6 | Alive |
7 | F | 24 | Bone (right femur),External ear (right) | - | 10 GY for femur,10 gy for ear | - | 6 | Alive |
8 | M | 24 | Bone (Right frontal, right femur),Lung | Cladribine (6 courses) | 5x190 cgy for frontal bone,1080 gy for femur | - | 3 | Alive |
Conclusion
LCH is a rare and heterogeneous disease of adult patients. Systemic evaluation is crucial because treatment desicion depends on organ-tissue involvement. Treatment should be individualized and multi-disciplinary in order to reach good outcome.
Session topic: 16. Myeloproliferative neoplasms - Clinical
Keyword(s): adult, Cladribine, Langerhans Cell Histiocytosis, Radiotherapy
Abstract: PB2279
Type: Publication Only
Background
Langerhans cell histiyocytosis (LCH) is a rare disease of histiocytes that is more prevalent in childhood. The etiology is unknown. Any organ or system may be affected in LCH. Bones, skin, and pituitary gland are frequently involved. Clinical presentation may be diverse according to the organ affected. Treatment modality depends on the extent of the disease. With mild symptoms and no risk organ involvement methotraxate, azathiopurin, thalidomide can be used or patient can be carefully observed without therapy. Symptomatic and mutisystemic LCH with or without risk organ involvement require chemotherapy.
Aims
Our aim is to evaluate clinical characteristics and outcome of adult onset LCH patients in our instutition.
Methods
We retrospectively evaluated adult patients diagnosed as LCH at Ege University Hospital between 2000-2017. All patients were screened by total bone X-ray survey and/or bone scintigraphy, abdominal and chest computerized tomography , cranial magnetic resonance imaging and some of the patients by positron emission tomography. Bone marrow aspiration and biopsy were performed in all patients in order to evaluate the possible bone marrow infiltration. Complete blood count, blood chemistry, erythrocyte sedimentation rate, coagulation studies, thyroid stimulating hormone and free T4, other pituitary gland hormones if pituitary gland is involved, and urine strip test were analyzed. Patients were stratified according to extent of the disease:Single system LCH (SS-LCH): One organ or system involved. It may be uni- or multifocal,Multisystem LCH (MS-LCH): Two or more organs/systems involved.Choice of treatment, dose and duration of drugs, radiotherapy fields and dosage, side effects of the treatment modalities were recorded. Outcome of the patients were evaluated.
Results
A total of 27 patients were diagnosed and treated in our hospital. Mean age at diagnosis was 38.3 years, 19 of them were male. There were 8 patients with MS-LCH, 13 with unifocal SS-LCH, and 6 with multifocal SS-LCH. Patients' characteristics were summarized in the tables 1, 2 and 3. All of our patients are alive. There was only one treatment toxicity, diabetes insipidus, in a patient with pons and mastoid lesion after radiotherapy. Most of MS-LCH and multifocal SS-LCH patients received systemic treatment, whereas unifocal SS-LCH.
Table 1: Patient characteristics with MS-LCH
Patient No | Gender | Age | Involved organ/tissue | Chemotherapy | Radiotherapy | Treatment toxicity | Follow-up period (years) | Outcome |
1 | M | 36 | Lung,Skin | Cladribine (6 courses) | - | - | 4 | Alive |
2 | M | 40 | Thyroid,Gum | Chemotherapy for concomitant thyroidpapillary carcinoma | - | - | 3 | Alive |
3 | M | 32 | Skin,Gum | Cladribine (6 courses) | - | - | 12 | Alive |
4 | M | 38 | Bone (parietal),Lung | Cladribine (5 courses) | - | - | 1 | Alive |
5 | F | 47 | Bone (left mandible, left tibia),Pons,Lung | - | Pons-mastoid 10x2 gy,tibia 10x2 gy | Diabetes insipidus | 8 | Alive |
6 | F | 47 | Bone (left parietal, left femur),Skin | Cladribine (6 courses) | - | - | 6 | Alive |
7 | F | 24 | Bone (right femur),External ear (right) | - | 10 GY for femur,10 gy for ear | - | 6 | Alive |
8 | M | 24 | Bone (Right frontal, right femur),Lung | Cladribine (6 courses) | 5x190 cgy for frontal bone,1080 gy for femur | - | 3 | Alive |
Conclusion
LCH is a rare and heterogeneous disease of adult patients. Systemic evaluation is crucial because treatment desicion depends on organ-tissue involvement. Treatment should be individualized and multi-disciplinary in order to reach good outcome.
Session topic: 16. Myeloproliferative neoplasms - Clinical
Keyword(s): adult, Cladribine, Langerhans Cell Histiocytosis, Radiotherapy