

Contributions
Abstract: PB2264
Type: Publication Only
Background
Mastocytosis is a rare disease, classically included in the myeloproliferative diseases, and characterized by clonal proliferation of mast cells (MCs) in one or more organs. In the WHO classification of 2016 it is a separate entity. There are two types, cutaneous mastocytosis (CM), affecting exclusively the skin, and systemic mastocytosis (SM), affecting mainly the bone marrow, among other organs. Clinical expressions are due to the anomalous release of mast cell mediators (MCMs) or to the infiltration of MCs into the tissues. MCs release a large amount of mediators during their activation, tryptase, histamine and heparin being the most specific elements which are also measurable in the conventional laboratory. Tryptase is produced almost exclusively by MCs, although it can also be increased in anaphylaxis, myeloid neoplasms and severe renal failure. Normal levels of it are almost undetectable in healthy individuals, up to 11.4 µg/L being normal. Levels >20 µg/L are one of the WHO’s minor criteria for the SM diagnosis.
Aims
To evaluate the diagnostic utility of increased levels of typtase as an independent marker in the diagnosis of SM
Methods
We retrospectively reviewed the 2.877 requests for bone marrow biopsy (BMB) addressed to the Department of Hematology in our hospital between March, 2009 and February, 2017, we selected those whose reason for request was elevated levels of tryptase
Results
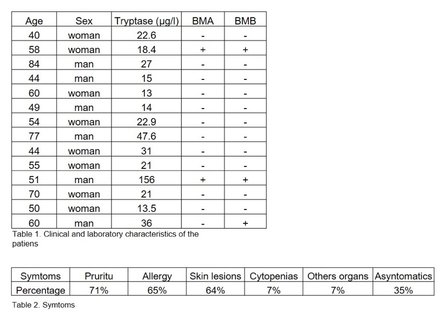
BMB were performed in 14 patients to rule out SM because of increase of tryptase levels. All these requests came from the Department of Allergy. Of the 14 cases 6 were male and 8 females, with a median age of 57 years old (Table 1). A review of medical records showed that 35% of the patients (5/14) did not present any other indication suggesting SM. The remaining 65% had a past history of allergy: medication (4), chronic urticaria (1), hymenoptera (1), food (1), sun allergy (1), metal (1). In addition, these patients presented different types of skin lesions (Table 2). Serum tryptase levels ranged between 13.5-156 µg/L (mean 32.7), and 10/14 (71%) showed levels >20 µg/L. The BMB was diagnostic of SM in 3/14 (21%). In these cases, atypical MCs were observed in the bone marrow aspirate (BMA), and they were positive for the KIT D816V mutation with an inmunophenotype CD59+, CD25+ and/or CD2+ by flow cytometry. Only 2/3 had tryptase levels >20 µg/L. These 3 cases, in addition to the elevated tryptase levels, had monoclonal IgG kappa and bone lesions. One case had diagnosis of CM before SM and another case had abnormal blood count. SM was not diagnosed in any case with elevated tryptase levels as the only abnormal parameter
Conclusion
In the light of our results, we can conclude that tryptase is a sensitive but not a specific marker for the diagnosis of SM. In the absence of any other clinical evidence, and with slightly elevated tryptase levels, the risk of having SM is very low, so the study of BMB is not useful and could be avoided, while the association of other data suggestive of SM or an increase of other MSMs confers a high risk of suffering SM
Session topic: 15. Myeloproliferative neoplasms – Biology & Translational Research
Keyword(s): Bone marrow biopsy, Diagnosis, Mastocytosis
Abstract: PB2264
Type: Publication Only
Background
Mastocytosis is a rare disease, classically included in the myeloproliferative diseases, and characterized by clonal proliferation of mast cells (MCs) in one or more organs. In the WHO classification of 2016 it is a separate entity. There are two types, cutaneous mastocytosis (CM), affecting exclusively the skin, and systemic mastocytosis (SM), affecting mainly the bone marrow, among other organs. Clinical expressions are due to the anomalous release of mast cell mediators (MCMs) or to the infiltration of MCs into the tissues. MCs release a large amount of mediators during their activation, tryptase, histamine and heparin being the most specific elements which are also measurable in the conventional laboratory. Tryptase is produced almost exclusively by MCs, although it can also be increased in anaphylaxis, myeloid neoplasms and severe renal failure. Normal levels of it are almost undetectable in healthy individuals, up to 11.4 µg/L being normal. Levels >20 µg/L are one of the WHO’s minor criteria for the SM diagnosis.
Aims
To evaluate the diagnostic utility of increased levels of typtase as an independent marker in the diagnosis of SM
Methods
We retrospectively reviewed the 2.877 requests for bone marrow biopsy (BMB) addressed to the Department of Hematology in our hospital between March, 2009 and February, 2017, we selected those whose reason for request was elevated levels of tryptase
Results
BMB were performed in 14 patients to rule out SM because of increase of tryptase levels. All these requests came from the Department of Allergy. Of the 14 cases 6 were male and 8 females, with a median age of 57 years old (Table 1). A review of medical records showed that 35% of the patients (5/14) did not present any other indication suggesting SM. The remaining 65% had a past history of allergy: medication (4), chronic urticaria (1), hymenoptera (1), food (1), sun allergy (1), metal (1). In addition, these patients presented different types of skin lesions (Table 2). Serum tryptase levels ranged between 13.5-156 µg/L (mean 32.7), and 10/14 (71%) showed levels >20 µg/L. The BMB was diagnostic of SM in 3/14 (21%). In these cases, atypical MCs were observed in the bone marrow aspirate (BMA), and they were positive for the KIT D816V mutation with an inmunophenotype CD59+, CD25+ and/or CD2+ by flow cytometry. Only 2/3 had tryptase levels >20 µg/L. These 3 cases, in addition to the elevated tryptase levels, had monoclonal IgG kappa and bone lesions. One case had diagnosis of CM before SM and another case had abnormal blood count. SM was not diagnosed in any case with elevated tryptase levels as the only abnormal parameter
Conclusion
In the light of our results, we can conclude that tryptase is a sensitive but not a specific marker for the diagnosis of SM. In the absence of any other clinical evidence, and with slightly elevated tryptase levels, the risk of having SM is very low, so the study of BMB is not useful and could be avoided, while the association of other data suggestive of SM or an increase of other MSMs confers a high risk of suffering SM
Session topic: 15. Myeloproliferative neoplasms – Biology & Translational Research
Keyword(s): Bone marrow biopsy, Diagnosis, Mastocytosis