

Contributions
Abstract: PB2254
Type: Publication Only
Background
Patients with relapsed and refractory multiple myeloma (MM) have poor prognosis. Life expectancy is increasing because of a rising number of agents with various mechanisms of action. However, MM remains incurable because of the emergence of resistant clones. Among these drugs, Daratumumab (DARA) is the first-in-class human monoclonal antibody against CD38 cells showing an overall response rate of 36% and a median overall survival (OS) of 17 months in monotherapy, now it can be used in combination with lenalidomide and dexamethasone, or bortezomib and dexamethasone, for the treatment of patients who have received at least one prior therapy. Ixazomib is a boron-containing selective proteasome inhibitor that demonstrated antimyeloma activity with excellent safety profile. Ixazomib is a proteasome inhibitor approved in combination with lenalidomide and dexamethasone for the treatment of patients who received at least one prior therapy.
Aims
We report two cases of relapsed MM treated with DARA-Ixazomib-Dexamethasone as rescue treatment, to our knowledge, the first study reporting this combination.
Methods
Description of two case reports about patients treated on our Unit.
Results
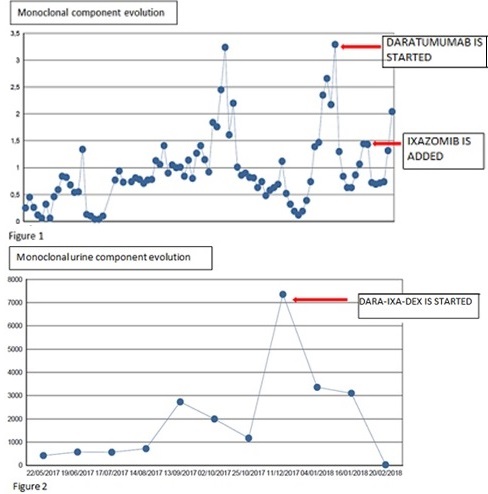
A 67-years-old woman with a known diagnosis of IgA lambda MM presented with relapsed MM. She first presented in 1999, was started on VBMCP/VBAD followed by auto transplant (ASCT), achieving a complete response (CR) but relapsed five years later, so she received bortezomib achieving a second CR. In 2007, a second relapsed was detected and she experimented a large sequence of treatment-relapsed consisting of VMP, Lenalidomide-dexamethasone, Bendamustine and Elotuzumab-thalidomide-dexamethasone. While the 13th cycle, she suffered a severe lung infection and was admitted in the critical care unit. Fortunately, she recovered well and was started on Carfilzomib. Next year, the disease progressed so we restarted Carfilzomib adding Dexamethasone (Kd), achieving a VGPR. Later, the disease progressed so the treatment was restarted but MM was refractory; in February 2017 a treatment based on DARA-bortezomib was initiated, but we stopped bortezomib because of severe neuropathy. After an optimal response, it got worse and Ixazomib was added; the disease evolution was optimal (Figure 1). After 12 cycles IgA levels increased slowly. At present, MM is in progression.
Our second case is a 60-years-old woman whose kappa light chain MM was detected in 2016, and was started on VTD achieving a good response, because of many complications, we stopped the treatment. After few months, she progressed so we started bortezomib-cyclofosphamide-dexamethasone (VCD) without response, so Rd was initiated. It was interrupted due to vertebral fractures. Promptly, she was started on Kd, but she debuted with a sepsis. After recovering, she received dexamethasone-cyclophosphamide-etoposide-cisplatin, but after one cycle she was diagnosed with a spinal cord compression. In December 2017, a regimen consisting of DARA 16mg/kg/week -Ixazomib 4 mg/week -dexamethasone was initiated. As striking decrease of the protein M in urine was observed (Figure 2), but a pancreatic plasmacytoma was detected. An ASCT was made and currently, after two months, MM is in a VGPR.
Conclusion
Daratumumab has shown benefit in patients who have progressed, and whose combination with other drugs just started to investigate. We combined this drug with Ixazomib in an attempt to control the disease, the response was good. However, optimization of the regimen could prolong response duration and improve patients' outcomes.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Monoclonal antibody, Multiple Myeloma, Proteasome inhibitor, Relapse
Abstract: PB2254
Type: Publication Only
Background
Patients with relapsed and refractory multiple myeloma (MM) have poor prognosis. Life expectancy is increasing because of a rising number of agents with various mechanisms of action. However, MM remains incurable because of the emergence of resistant clones. Among these drugs, Daratumumab (DARA) is the first-in-class human monoclonal antibody against CD38 cells showing an overall response rate of 36% and a median overall survival (OS) of 17 months in monotherapy, now it can be used in combination with lenalidomide and dexamethasone, or bortezomib and dexamethasone, for the treatment of patients who have received at least one prior therapy. Ixazomib is a boron-containing selective proteasome inhibitor that demonstrated antimyeloma activity with excellent safety profile. Ixazomib is a proteasome inhibitor approved in combination with lenalidomide and dexamethasone for the treatment of patients who received at least one prior therapy.
Aims
We report two cases of relapsed MM treated with DARA-Ixazomib-Dexamethasone as rescue treatment, to our knowledge, the first study reporting this combination.
Methods
Description of two case reports about patients treated on our Unit.
Results
A 67-years-old woman with a known diagnosis of IgA lambda MM presented with relapsed MM. She first presented in 1999, was started on VBMCP/VBAD followed by auto transplant (ASCT), achieving a complete response (CR) but relapsed five years later, so she received bortezomib achieving a second CR. In 2007, a second relapsed was detected and she experimented a large sequence of treatment-relapsed consisting of VMP, Lenalidomide-dexamethasone, Bendamustine and Elotuzumab-thalidomide-dexamethasone. While the 13th cycle, she suffered a severe lung infection and was admitted in the critical care unit. Fortunately, she recovered well and was started on Carfilzomib. Next year, the disease progressed so we restarted Carfilzomib adding Dexamethasone (Kd), achieving a VGPR. Later, the disease progressed so the treatment was restarted but MM was refractory; in February 2017 a treatment based on DARA-bortezomib was initiated, but we stopped bortezomib because of severe neuropathy. After an optimal response, it got worse and Ixazomib was added; the disease evolution was optimal (Figure 1). After 12 cycles IgA levels increased slowly. At present, MM is in progression.
Our second case is a 60-years-old woman whose kappa light chain MM was detected in 2016, and was started on VTD achieving a good response, because of many complications, we stopped the treatment. After few months, she progressed so we started bortezomib-cyclofosphamide-dexamethasone (VCD) without response, so Rd was initiated. It was interrupted due to vertebral fractures. Promptly, she was started on Kd, but she debuted with a sepsis. After recovering, she received dexamethasone-cyclophosphamide-etoposide-cisplatin, but after one cycle she was diagnosed with a spinal cord compression. In December 2017, a regimen consisting of DARA 16mg/kg/week -Ixazomib 4 mg/week -dexamethasone was initiated. As striking decrease of the protein M in urine was observed (Figure 2), but a pancreatic plasmacytoma was detected. An ASCT was made and currently, after two months, MM is in a VGPR.
Conclusion
Daratumumab has shown benefit in patients who have progressed, and whose combination with other drugs just started to investigate. We combined this drug with Ixazomib in an attempt to control the disease, the response was good. However, optimization of the regimen could prolong response duration and improve patients' outcomes.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Monoclonal antibody, Multiple Myeloma, Proteasome inhibitor, Relapse