

Contributions
Abstract: PB2436
Type: Publication Only
Background
Allogeneic hematopoietic stem cell transplantation (HSCT) is an effective therapy for a variety of malignant and non-malignant hematologic disorders. Myeloablative conditioning (MAC) and reduced-intensity conditioning (RIC) regimens may have different clinical outcomes. Several investigators have reported a dose-response relationship between the pretransplant conditioning regimen and long-term outcome after allogeneic hematopoietic transplantation in acute leukemia. MAC regimens are associated with a reduced risk of relapse after HSCT, but it’s doubtful. That it translates into prolongation of overall survival due to the increased treatment-related and nonrelapse mortality. In many studies, RIC has been shown to have similar overall survival (OS) but higher relapse rates compared with MAC regimens in patients with myeloid malignancies undergoing allogeneic HSCT.
Aims
To evaluate long-term outcome of MAC versus RIC regimens in patients with acute myeloid leukemia (AML) patients undergoing allogeneic HSCT.
Methods
This study is a retrospective single-center analysis. We retrospectively compared the long term outcome with MAC and RIC regimens in patients who underwent allo-HSCT for AML at Hacettepe University between 2001 and 2017.
Results
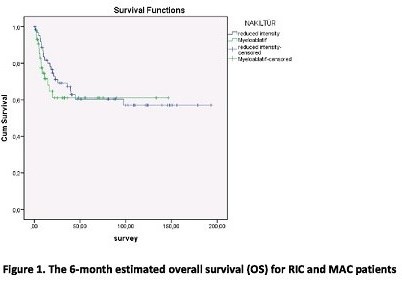
We analyzed the survival outcomes after MAC-HSCT versus RIC-HSCT among 107 adult patients with AML diagnosed from 2001 through 2017. Of these, 44 patients received a MAC regimen and 63 patients received a fludarabine-based RIC regimen in AML. Median follow-up of 95 months (range, 7-213) for the RIC-HCT group and 34 months (range, 6-153) for the MAC-HCT group. The 6-month estimated survival was found to be higher in RIC patients as compared to MAC patients (93% versus %82), but no statistically significant difference was observed (p: 0,5). The 3-year estimated survival for RIC and MAC patients were 67 % and 60 %, respectively. In multivariate analysis, the type of conditioning regimen (RIC vs MAC) did not influence the progression free survival (p: 0,24). Five of the RIC patients and 9 of the MAC patients developed acute graft versus host disease (GvHD). Sixteen of the RIC patients and 6 of the MAC patients developed chronic GvHD. There was no significant difference between two groups in terms of acute and chronic GvHD (p: 0,089).
Conclusion
This retrospective analysis confirmed that MAC and RIC regimens had a consistently equivalent rate of overall and disease free survival in AML patients with allogeneic HSCT.
Session topic: 23. Stem cell transplantation - Clinical
Keyword(s): Acute Myeloid Leukemia, Allogeneic hematopoietic stem cell transplant, Regimen
Abstract: PB2436
Type: Publication Only
Background
Allogeneic hematopoietic stem cell transplantation (HSCT) is an effective therapy for a variety of malignant and non-malignant hematologic disorders. Myeloablative conditioning (MAC) and reduced-intensity conditioning (RIC) regimens may have different clinical outcomes. Several investigators have reported a dose-response relationship between the pretransplant conditioning regimen and long-term outcome after allogeneic hematopoietic transplantation in acute leukemia. MAC regimens are associated with a reduced risk of relapse after HSCT, but it’s doubtful. That it translates into prolongation of overall survival due to the increased treatment-related and nonrelapse mortality. In many studies, RIC has been shown to have similar overall survival (OS) but higher relapse rates compared with MAC regimens in patients with myeloid malignancies undergoing allogeneic HSCT.
Aims
To evaluate long-term outcome of MAC versus RIC regimens in patients with acute myeloid leukemia (AML) patients undergoing allogeneic HSCT.
Methods
This study is a retrospective single-center analysis. We retrospectively compared the long term outcome with MAC and RIC regimens in patients who underwent allo-HSCT for AML at Hacettepe University between 2001 and 2017.
Results
We analyzed the survival outcomes after MAC-HSCT versus RIC-HSCT among 107 adult patients with AML diagnosed from 2001 through 2017. Of these, 44 patients received a MAC regimen and 63 patients received a fludarabine-based RIC regimen in AML. Median follow-up of 95 months (range, 7-213) for the RIC-HCT group and 34 months (range, 6-153) for the MAC-HCT group. The 6-month estimated survival was found to be higher in RIC patients as compared to MAC patients (93% versus %82), but no statistically significant difference was observed (p: 0,5). The 3-year estimated survival for RIC and MAC patients were 67 % and 60 %, respectively. In multivariate analysis, the type of conditioning regimen (RIC vs MAC) did not influence the progression free survival (p: 0,24). Five of the RIC patients and 9 of the MAC patients developed acute graft versus host disease (GvHD). Sixteen of the RIC patients and 6 of the MAC patients developed chronic GvHD. There was no significant difference between two groups in terms of acute and chronic GvHD (p: 0,089).
Conclusion
This retrospective analysis confirmed that MAC and RIC regimens had a consistently equivalent rate of overall and disease free survival in AML patients with allogeneic HSCT.
Session topic: 23. Stem cell transplantation - Clinical
Keyword(s): Acute Myeloid Leukemia, Allogeneic hematopoietic stem cell transplant, Regimen