

Contributions
Abstract: S1582
Type: Oral Presentation
Presentation during EHA23: On Sunday, June 17, 2018 from 08:30 - 08:45
Location: Room A8
Background
Severe Congenital Neutropenia (SCN) due to ELANE mutations is usually managed with Granulocyte–Colony Stimulating Factor (G-CSF) but may also be amenable for treatment with Allogeneic Haematopoietic Stem Cell Transplantation (HSCT). According to the experts, HSCT is indicated in patients transformed into MDS/AL or who are refractory/poor responding to G-CSF (> 20 mcg/kg/day). HSCT looks also appropriate for those subjects treated with G-CSF at doses between 10-20 mcg/kg/d, while the indications for those subjects managed with doses up to 10 mcg/kg are less clear.
Aims
To retrospectively compare the long term outcome of SCN-ELANE patients who underwent HCST vs those who did not, stratified according to G-CSF dose .
Methods
Data have been extracted from the Severe Chronic Neutropenia French registry (SCNFR), the Italian Neutropenia Registry (INR), from the database of the Severe Aplastic Anemia Working Group of the European Society for Blood and Marrow Transplantation (EBMT) and from Stem Cell Transplant for Immunodeficiencies in Europe (SCETIDE) in the years 1990-2017. The received dose of G-CSF was estimated by calculating the amount of drug that patients received for more than 75% of the treatment time (when daily dose was not available for the whole treatment period) or by calculating the mean dose (total amount/days of treatment) whenever daily dose was available for the full period. The cohort has been arbitrarly stratified in two subgroups according to the dose of G-CSF received: ≤10 mcg/kg/d, and >10 mcg/kg/d.
Results
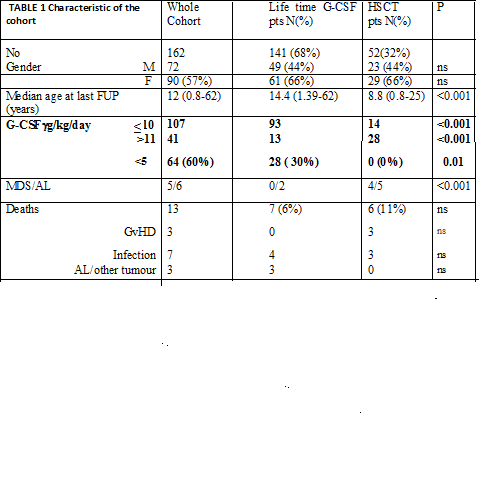
162 SCN ELANE patients were considered eligible for the study, 141 were treated with G-CSF and 52 received HSCT. Transplant indication was as per Center policy. Characteristics of the population are shown in Table 1. The 15 y-OS of the whole group was 91% (95% IC; 84-95). HSCT patients had worse survival vs those treated with G-CSF: 79% (95% IC; 52-92) vs 94% (95% IC 87-97) respectively (p=0.031). The 15y-OS of patients receiving G-CSF >11mcg/kg/d was 85% (95% IC; 51-96) vs 74% (95% IC 33-92) of HSCT patients (p 0.325). Transplanted patients receiving ≤ 10mcg/kg/d of G-CSF had significantly lower 15-yr OS if compared with the G-CSF treated subjects (74% -95% IC 24-94 vs 98% -95% IC 91-99-) (p=0.015). In the subgroup treated with G-CSF ≤ 10mcg/kg/d who underwent HSCT, 1 patients had AL, 1 had unmanageable infections and 5 had available an identical siblings. Comparison of OS in the two groups by additional “risk factors” other than CSF dose is ongoing.
Conclusion
This is the largest comparative analysis between HSCT and life-time G-CSF conducted in ELANE-SCN cohort . The OS of the whole cohort 91 % after 15 y of follow up. On the whole the HSCT group shows a significantly worse survival vs G-CSF treated one probably because a negative selection of the transplanted patients . However the OS of the group who received G-CSF ≤10mcg/kg/d and underwent HSCT was significantly inferior than that managed with G-CSF alone . This suggests that indication to transplant for patients receiving G-CSF dose ≤10mcg/kg/d needs to be carefully balanced. Definitive conclusion might be drawn at the completion of analysis including other factors that may affect the outcome like molecular characteristics, clonal evolution markers and infection load.
Session topic: 12. Bone marrow failure syndromes incl. PNH - Clinical
Keyword(s): Granulocyte colony-stimulating factor (G-CSF), Severe congenital neutropenia, Stem cell transplant
Abstract: S1582
Type: Oral Presentation
Presentation during EHA23: On Sunday, June 17, 2018 from 08:30 - 08:45
Location: Room A8
Background
Severe Congenital Neutropenia (SCN) due to ELANE mutations is usually managed with Granulocyte–Colony Stimulating Factor (G-CSF) but may also be amenable for treatment with Allogeneic Haematopoietic Stem Cell Transplantation (HSCT). According to the experts, HSCT is indicated in patients transformed into MDS/AL or who are refractory/poor responding to G-CSF (> 20 mcg/kg/day). HSCT looks also appropriate for those subjects treated with G-CSF at doses between 10-20 mcg/kg/d, while the indications for those subjects managed with doses up to 10 mcg/kg are less clear.
Aims
To retrospectively compare the long term outcome of SCN-ELANE patients who underwent HCST vs those who did not, stratified according to G-CSF dose .
Methods
Data have been extracted from the Severe Chronic Neutropenia French registry (SCNFR), the Italian Neutropenia Registry (INR), from the database of the Severe Aplastic Anemia Working Group of the European Society for Blood and Marrow Transplantation (EBMT) and from Stem Cell Transplant for Immunodeficiencies in Europe (SCETIDE) in the years 1990-2017. The received dose of G-CSF was estimated by calculating the amount of drug that patients received for more than 75% of the treatment time (when daily dose was not available for the whole treatment period) or by calculating the mean dose (total amount/days of treatment) whenever daily dose was available for the full period. The cohort has been arbitrarly stratified in two subgroups according to the dose of G-CSF received: ≤10 mcg/kg/d, and >10 mcg/kg/d.
Results
162 SCN ELANE patients were considered eligible for the study, 141 were treated with G-CSF and 52 received HSCT. Transplant indication was as per Center policy. Characteristics of the population are shown in Table 1. The 15 y-OS of the whole group was 91% (95% IC; 84-95). HSCT patients had worse survival vs those treated with G-CSF: 79% (95% IC; 52-92) vs 94% (95% IC 87-97) respectively (p=0.031). The 15y-OS of patients receiving G-CSF >11mcg/kg/d was 85% (95% IC; 51-96) vs 74% (95% IC 33-92) of HSCT patients (p 0.325). Transplanted patients receiving ≤ 10mcg/kg/d of G-CSF had significantly lower 15-yr OS if compared with the G-CSF treated subjects (74% -95% IC 24-94 vs 98% -95% IC 91-99-) (p=0.015). In the subgroup treated with G-CSF ≤ 10mcg/kg/d who underwent HSCT, 1 patients had AL, 1 had unmanageable infections and 5 had available an identical siblings. Comparison of OS in the two groups by additional “risk factors” other than CSF dose is ongoing.
Conclusion
This is the largest comparative analysis between HSCT and life-time G-CSF conducted in ELANE-SCN cohort . The OS of the whole cohort 91 % after 15 y of follow up. On the whole the HSCT group shows a significantly worse survival vs G-CSF treated one probably because a negative selection of the transplanted patients . However the OS of the group who received G-CSF ≤10mcg/kg/d and underwent HSCT was significantly inferior than that managed with G-CSF alone . This suggests that indication to transplant for patients receiving G-CSF dose ≤10mcg/kg/d needs to be carefully balanced. Definitive conclusion might be drawn at the completion of analysis including other factors that may affect the outcome like molecular characteristics, clonal evolution markers and infection load.
Session topic: 12. Bone marrow failure syndromes incl. PNH - Clinical
Keyword(s): Granulocyte colony-stimulating factor (G-CSF), Severe congenital neutropenia, Stem cell transplant