

Contributions
Abstract: S142
Type: Oral Presentation
Presentation during EHA23: On Friday, June 15, 2018 from 12:15 - 12:30
Location: Room A9
Background
Abnormal bleeding is a common complication of systemic Amyloidosis. Proposed mechanisms include Amyloid angiopathy and coagulation abnormalities among which Factor X deficiency is the most common. Prolongation of prothrombin time (PT) and partial thromboplastin time (PTT) were also reported.
Aims
We performed a retrospective review of different coagulation factors of systemic Amyloidosis patients from the Amyloid Database at the Houston Methodist Hospital between 2006 and 2015 to investigate the mechanisms of abnormal bleeding.
Methods
The patient data was queried from METEOR (Methodist Environment for Translational Enhancement and Outcomes Research), a clinical data warehouse that contains records dating back to January 1, 2006. We queried for the diagnosis of systemic Amyloidosis, clinically significant bleeding events, coagulation factors and other laboratory results along with patient demographics. The diagnosis of systemic Amyloidosis was further confirmed by reviewing tissue biopsy reports. The degree of bleeding was categorized into 4 grades according to World Health Organization standardized grading scale. Grade 2 or higher was defined as clinically significant bleeding. Grade 3 or 4 was considered as severe bleeding. Laboratory data including Factor X activity, PT, PTT, international normalized ratio (INR), platelets and fibrinogen were reviewed. Average laboratory test values in each clinical visit were used in univariate logistic regression test to investigate association of coagulation abnormalities with clinical significant bleeding and severe bleeding events.
Results
230 patients and 2178 encounters were identified after excluding patients on anticoagulation. The type of the Amyloidosis was confirmed in 168 patients, 148 of which are primary Amyloidosis with the rest listed as unknown. 26 patients had at least one clinically significant bleeding event.
140 patients had PT and INR measured; 138 patients had PTT measured; 162 patients had platelet measured; 48 patients had fibrinogen measured and 34 had Factor X level measured.
Elevated PT and INR were identified in 86/140 (61%) patients, elevated PTT in 61/138 (44%) patients, thrombocytopenia in 79/162 (48%) patients, abnormal Factor X (<70%) in 19/34 (56%) patients and decreased fibrinogen level (< 200) in 5/48 (11%) patients.
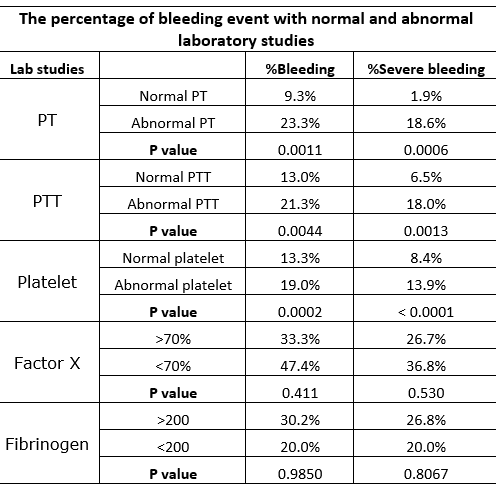
In univariate logistic regression analysis, prolongation of PT, INR, PTT and thrombocytopenia were independent variables associated with clinically significant bleeding (p=0.0011, p=0.0007, p=0.0044 and p= 0.0002 respectively). The same variables are also independently associated with severe bleeding events (p=0.0006, p=0.0004, p=0.0013 and p< 0.0001 respectively). Factor X and fibrinogen level were not significantly associated with clinically significant bleeding or severe bleeding events.
Conclusion
Prolonged PT, INR and PTT are common in systemic Amyloidosis and correlate with increased bleeding events. Factor X deficiency is common but contrary to observations from previous studies, no correlation of it with abnormal bleeding was seen in our review. This could be explained by our low number of Factor X measurements. Studies with systemic measurements of PT, PTT, platelet and factor X activity are needed to further investigate the bleeding mechanisms in systemic Amyloidosis.
Session topic: 34. Bleeding disorders (congenital and acquired)
Keyword(s): Amyloidosis, Bleeding, Coagulation
Abstract: S142
Type: Oral Presentation
Presentation during EHA23: On Friday, June 15, 2018 from 12:15 - 12:30
Location: Room A9
Background
Abnormal bleeding is a common complication of systemic Amyloidosis. Proposed mechanisms include Amyloid angiopathy and coagulation abnormalities among which Factor X deficiency is the most common. Prolongation of prothrombin time (PT) and partial thromboplastin time (PTT) were also reported.
Aims
We performed a retrospective review of different coagulation factors of systemic Amyloidosis patients from the Amyloid Database at the Houston Methodist Hospital between 2006 and 2015 to investigate the mechanisms of abnormal bleeding.
Methods
The patient data was queried from METEOR (Methodist Environment for Translational Enhancement and Outcomes Research), a clinical data warehouse that contains records dating back to January 1, 2006. We queried for the diagnosis of systemic Amyloidosis, clinically significant bleeding events, coagulation factors and other laboratory results along with patient demographics. The diagnosis of systemic Amyloidosis was further confirmed by reviewing tissue biopsy reports. The degree of bleeding was categorized into 4 grades according to World Health Organization standardized grading scale. Grade 2 or higher was defined as clinically significant bleeding. Grade 3 or 4 was considered as severe bleeding. Laboratory data including Factor X activity, PT, PTT, international normalized ratio (INR), platelets and fibrinogen were reviewed. Average laboratory test values in each clinical visit were used in univariate logistic regression test to investigate association of coagulation abnormalities with clinical significant bleeding and severe bleeding events.
Results
230 patients and 2178 encounters were identified after excluding patients on anticoagulation. The type of the Amyloidosis was confirmed in 168 patients, 148 of which are primary Amyloidosis with the rest listed as unknown. 26 patients had at least one clinically significant bleeding event.
140 patients had PT and INR measured; 138 patients had PTT measured; 162 patients had platelet measured; 48 patients had fibrinogen measured and 34 had Factor X level measured.
Elevated PT and INR were identified in 86/140 (61%) patients, elevated PTT in 61/138 (44%) patients, thrombocytopenia in 79/162 (48%) patients, abnormal Factor X (<70%) in 19/34 (56%) patients and decreased fibrinogen level (< 200) in 5/48 (11%) patients.
In univariate logistic regression analysis, prolongation of PT, INR, PTT and thrombocytopenia were independent variables associated with clinically significant bleeding (p=0.0011, p=0.0007, p=0.0044 and p= 0.0002 respectively). The same variables are also independently associated with severe bleeding events (p=0.0006, p=0.0004, p=0.0013 and p< 0.0001 respectively). Factor X and fibrinogen level were not significantly associated with clinically significant bleeding or severe bleeding events.
Conclusion
Prolonged PT, INR and PTT are common in systemic Amyloidosis and correlate with increased bleeding events. Factor X deficiency is common but contrary to observations from previous studies, no correlation of it with abnormal bleeding was seen in our review. This could be explained by our low number of Factor X measurements. Studies with systemic measurements of PT, PTT, platelet and factor X activity are needed to further investigate the bleeding mechanisms in systemic Amyloidosis.
Session topic: 34. Bleeding disorders (congenital and acquired)
Keyword(s): Amyloidosis, Bleeding, Coagulation