

Contributions
Abstract: PB2163
Type: Publication Only
Background
Primary amyloidosis (AL) is characterized by extracellular deposition of insoluble protein fibrils often with multisystem organ involvement. The Mayo staging model for determining prognosis in patients with cardiac amyloidosis takes into account troponin, NT-proBNP, and serum free-light chain difference in order to stage patients prior to undergoing autologous hematopoietic stem cell transplant (Auto-HCT). Since amyloidosis often involves the kidneys, serum biomarkers that require renal clearance are less reliable in the setting of significant renal dysfunction. 2D-echo and strain imaging offer non-invasive modalities for identifying early cardiac changes independent of renal function. These changes may also precede symptom improvement as assessed by NYHA classification.
Aims
Our hypothesis is that strain imaging is a feasible biomarker for cardiac respone after Auto-HCT in AL amyloidosis
Methods
Seven patients with biopsy-proven AL amyloidosis who were treated with a Melphalan based myeloablative regimen and Auto-HCT were evaluated retrospectively. Each patient underwent 2D-echo up to 36-days prior to treatment followed by repeat 2D-echo within 14-months. Strain imaging was performed using EchoInsight®. Chart review was conducted to determine associated NYHA functional classification and Mayo staging. Statistical analysis was performed using SPSS.
Results
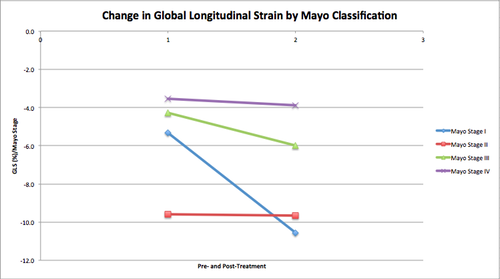
Of the 7 patients studied, 3 were Mayo stage I, 2 stage II, 1 stage III, and 1 stage IV. The median follow-up from transplant was 47.4 months. There was one death at 20.4 months. The mean NYHA classification at baseline was 2.3 and after transplant was 1.9. Longitudinal, radial and circumferential left ventricular strain (LV) were evaluated, but only the global longitudinal strain (GLS) showed an improvement (baseline -14.69%; follow-up -16.84%; mean absolute improvement 2.15%; p < 0.05) across all four Mayo Stages. There was no difference in GLS within individual stages. In patients with stable NYHA classification after transplant, there was also a significant improvement in Right Ventricular Free-Wall Strain (RVFWS) with a mean absolute improvement of 6.2% (p < 0.05). There was no significant change in left ventricular ejection fraction (LVEF).
Conclusion
We demonstrate that there is a clinically meaningful improvement in cardiac mechanics one year after Auto-HCT, despite no alteration in LVEF. This metric may prove useful in assessing organ response, especially when serum biomarkers are less reliable. Changes in left ventricular GLS occur independent of pre-transplant Mayo stage, although prospective studies are needed for confirmation. We further believe that improvements in RVFWS may predict clinical improvement.
Session topic: 22. Stem cell transplantation - Clinical
Keyword(s): AL amyloidosis
Abstract: PB2163
Type: Publication Only
Background
Primary amyloidosis (AL) is characterized by extracellular deposition of insoluble protein fibrils often with multisystem organ involvement. The Mayo staging model for determining prognosis in patients with cardiac amyloidosis takes into account troponin, NT-proBNP, and serum free-light chain difference in order to stage patients prior to undergoing autologous hematopoietic stem cell transplant (Auto-HCT). Since amyloidosis often involves the kidneys, serum biomarkers that require renal clearance are less reliable in the setting of significant renal dysfunction. 2D-echo and strain imaging offer non-invasive modalities for identifying early cardiac changes independent of renal function. These changes may also precede symptom improvement as assessed by NYHA classification.
Aims
Our hypothesis is that strain imaging is a feasible biomarker for cardiac respone after Auto-HCT in AL amyloidosis
Methods
Seven patients with biopsy-proven AL amyloidosis who were treated with a Melphalan based myeloablative regimen and Auto-HCT were evaluated retrospectively. Each patient underwent 2D-echo up to 36-days prior to treatment followed by repeat 2D-echo within 14-months. Strain imaging was performed using EchoInsight®. Chart review was conducted to determine associated NYHA functional classification and Mayo staging. Statistical analysis was performed using SPSS.
Results
Of the 7 patients studied, 3 were Mayo stage I, 2 stage II, 1 stage III, and 1 stage IV. The median follow-up from transplant was 47.4 months. There was one death at 20.4 months. The mean NYHA classification at baseline was 2.3 and after transplant was 1.9. Longitudinal, radial and circumferential left ventricular strain (LV) were evaluated, but only the global longitudinal strain (GLS) showed an improvement (baseline -14.69%; follow-up -16.84%; mean absolute improvement 2.15%; p < 0.05) across all four Mayo Stages. There was no difference in GLS within individual stages. In patients with stable NYHA classification after transplant, there was also a significant improvement in Right Ventricular Free-Wall Strain (RVFWS) with a mean absolute improvement of 6.2% (p < 0.05). There was no significant change in left ventricular ejection fraction (LVEF).
Conclusion
We demonstrate that there is a clinically meaningful improvement in cardiac mechanics one year after Auto-HCT, despite no alteration in LVEF. This metric may prove useful in assessing organ response, especially when serum biomarkers are less reliable. Changes in left ventricular GLS occur independent of pre-transplant Mayo stage, although prospective studies are needed for confirmation. We further believe that improvements in RVFWS may predict clinical improvement.
Session topic: 22. Stem cell transplantation - Clinical
Keyword(s): AL amyloidosis