
A RETROSPECTIVE AND PROSPECTIVE AUDIT OF RADIOLOGICAL INVESTIGATIONS FOR SUSPECTED CASES OF PLASMA CELL DYSCRASIAS/MYELOMA IN THE ALTNAGELVIN AREA HOSPITAL
(Abstract release date: 05/18/17)
EHA Library. Baker G. 05/18/17; 182731; PB2017

Gavin Baker
Contributions
Contributions
Abstract
Abstract: PB2017
Type: Publication Only
Background
The updated NICE guidelines for diagnosis and management of myeloma (2016) suggests whole-body MRI as first-line imaging for people with suspected myeloma and consideration of MRI/CT/PET in newly diagnosed myeloma to assess for bone disease or EM plasmacytoma.
Aims
Our aims were to ascertian; 1) Our current practice regarding radiological investigation for myeloma
(2) Whether additional diagnostic information was gained using CT/MRI imaging
(3) Since its release, is the trust compliant with the NICE guidance
(4) The estimated cost of meeting the current NICE guidance
Methods
This retrospective and prospective audit included all patients having a skeletal survey performed for suspected multiple myeloma within the Altnagelvin Area Hospital (AAH). Retrospectively from 10/2/15 until 9/2/16 data was collected using the advanced search feature of the Sectra IDS7 PACS system. The ‘Reason for examination’ for each study was then analysed and those ordered for reasons other than suspected myeloma were excluded. Each case was analysed individually and any follow up MRI/CT/NMB imaging performed in the 6 month period following the skeletal survey were included in the data collection. The same information was gathered prospectively from 10/2/16-30/5/16 following the NICE guidance. 54 skeletal surveys where performed for suspected/restaging myeloma pre guidance.
Results
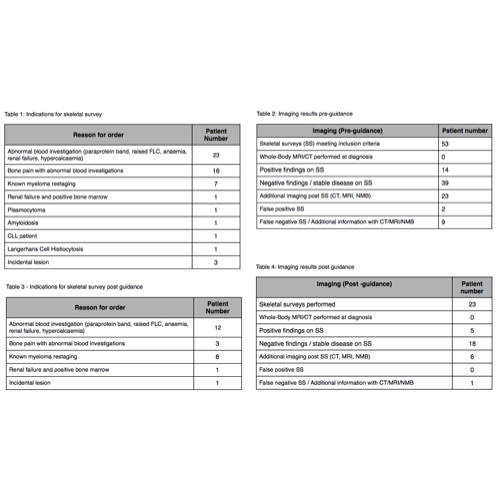
The indications for requesting imaging is shown in Table 1. No WB MRI/CT was performed in this period. 26% patients had new lytic lesions on skeletal survey. 23 patients had further imaging in the form of MRI or CT following skeletal surveys. All the positive MRI findings offered additional diagnostic information - including examples of missed multiple spinal deposits. The results of imaging are summarised in Table 2. The false negative rate for skeletal surveys was 39% and the false positive rate was 22%.
Following NICE guidance publication 23 patients had skeletal surveys performed for suspicion of myeloma between 10/2/16 and 30/5/16. The indications are summarised in Table 3. No WB imaging was performed. 5 patients had positive skeletal surveys. 6 patients had subsequent CT/ MRI imaging. A skeletal survey was reported normal with a subsequent MRI showing multiple spinal deposits. The imaging results are summarised in Table 4.
Conclusion
The expected cost of implementing WB imaging for 60 patients per year in the AAH is £18,240. In comparison the cost of performing skeletal surveys would be £4200 per annum. NICE guidance 2016 offers an economic model for imaging with WB MRI. In addition it reviews evidence which links time to diagnosis to survival and myeloma related complications. The NICE guidance offers clear evidence that WB-MRI should be the investigation modality of choice for suspected myelomatous disease. It offers a diagnostic and cost-effective strategy that will ensure health improvements for myeloma patients.
This audit offers further evidence of the diagnostic accuracy of MRI imaging. At present failure to comply with NICE guidance will lead to delayed diagnosis of myeloma in certain patients and potential patient harm. Therefore I offer a business and health improvement case for the Western Trust to instigate WB-MRI imaging for all suspected myelomatous bony disease.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Diagnosis, Myeloma, MRI
Abstract: PB2017
Type: Publication Only
Background
The updated NICE guidelines for diagnosis and management of myeloma (2016) suggests whole-body MRI as first-line imaging for people with suspected myeloma and consideration of MRI/CT/PET in newly diagnosed myeloma to assess for bone disease or EM plasmacytoma.
Aims
Our aims were to ascertian; 1) Our current practice regarding radiological investigation for myeloma
(2) Whether additional diagnostic information was gained using CT/MRI imaging
(3) Since its release, is the trust compliant with the NICE guidance
(4) The estimated cost of meeting the current NICE guidance
Methods
This retrospective and prospective audit included all patients having a skeletal survey performed for suspected multiple myeloma within the Altnagelvin Area Hospital (AAH). Retrospectively from 10/2/15 until 9/2/16 data was collected using the advanced search feature of the Sectra IDS7 PACS system. The ‘Reason for examination’ for each study was then analysed and those ordered for reasons other than suspected myeloma were excluded. Each case was analysed individually and any follow up MRI/CT/NMB imaging performed in the 6 month period following the skeletal survey were included in the data collection. The same information was gathered prospectively from 10/2/16-30/5/16 following the NICE guidance. 54 skeletal surveys where performed for suspected/restaging myeloma pre guidance.
Results
The indications for requesting imaging is shown in Table 1. No WB MRI/CT was performed in this period. 26% patients had new lytic lesions on skeletal survey. 23 patients had further imaging in the form of MRI or CT following skeletal surveys. All the positive MRI findings offered additional diagnostic information - including examples of missed multiple spinal deposits. The results of imaging are summarised in Table 2. The false negative rate for skeletal surveys was 39% and the false positive rate was 22%.
Following NICE guidance publication 23 patients had skeletal surveys performed for suspicion of myeloma between 10/2/16 and 30/5/16. The indications are summarised in Table 3. No WB imaging was performed. 5 patients had positive skeletal surveys. 6 patients had subsequent CT/ MRI imaging. A skeletal survey was reported normal with a subsequent MRI showing multiple spinal deposits. The imaging results are summarised in Table 4.
Conclusion
The expected cost of implementing WB imaging for 60 patients per year in the AAH is £18,240. In comparison the cost of performing skeletal surveys would be £4200 per annum. NICE guidance 2016 offers an economic model for imaging with WB MRI. In addition it reviews evidence which links time to diagnosis to survival and myeloma related complications. The NICE guidance offers clear evidence that WB-MRI should be the investigation modality of choice for suspected myelomatous disease. It offers a diagnostic and cost-effective strategy that will ensure health improvements for myeloma patients.
This audit offers further evidence of the diagnostic accuracy of MRI imaging. At present failure to comply with NICE guidance will lead to delayed diagnosis of myeloma in certain patients and potential patient harm. Therefore I offer a business and health improvement case for the Western Trust to instigate WB-MRI imaging for all suspected myelomatous bony disease.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Diagnosis, Myeloma, MRI
{{ help_message }}
{{filter}}