

Contributions
Abstract: PB2008
Type: Publication Only
Background
Plasma cell leukaemia (PCL) is a rare and aggressive plasma cell (PC) disorder characterized by the presence of circulating plasma cells. PCL can either originate de novo (pPCL) or as secondary PCL (sPCL) in patients with relapsed/refractory multiple myeloma (MM). PCL has a more aggressive clinical presentation than MM with a more frequent extramedullary involvement, such as leptomeningeal infiltration. However, because of the low incidence of this entity, most clinical data come from small retrospective studies. Classical diagnosis criteria of PCL are today under review and the incidence of leptomeningeal infiltration is unknown.
Aims
We aimed to study the clinical features with special emphasis in the incidence leptomeningeal infiltration in patients diagnosed with PCL in our centre.
Methods
Results
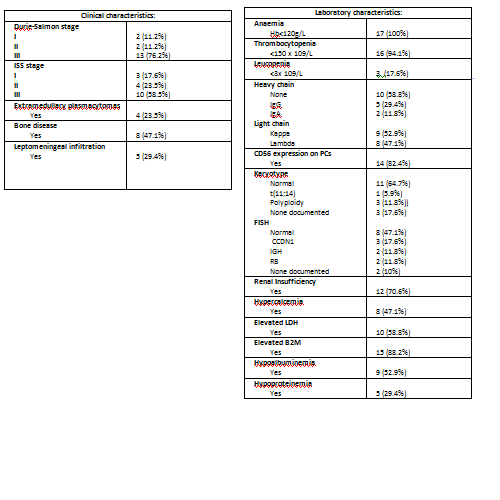
Seventeen patients with PCL were included. Six (35.3%) were pPCL and eleven (64.7%) sPCL. Median age at diagnosis was 57 years (range 35-78) and 8 (47.1%) were males. Clinical and analytical features at the moment of diagnosis are recorded in Table 1. Five (29.4%) patients presented with leptomeningeal infiltration; in three of them it was diagnosed at the time of the diagnosis of PCL. All the patients had neurological features. Thirteen (76.4%) patients were able to start a curative treatment: VD in 7 (53.8%) patients, VTD in 2 (15.4%), VAD in 1 (7.7%), D-PACE in 1, MTX-ARAC in 1 patient and RD in the remaining one. Three patients received intrathecal treatment. The intention-to-treat response was: 2 (15.4%) CR, 2 PR, 7 (53.9%) refractory disease/progression and 2 non-evaluable. Only 2 (15.4%) patients achieved enough response (2 CR) to undergo an autologous stem cell transplant (ACST) and only 1 to undergo an allogenic-SCT. With a median follow up of 4 months for all the patients inclosed, median of PFS was 3 (CI 95% 0.47-4.76) months and median of OS was 4 (IC 95% 0.47-7.53) months.
Conclusion
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Plasma cells
Abstract: PB2008
Type: Publication Only
Background
Plasma cell leukaemia (PCL) is a rare and aggressive plasma cell (PC) disorder characterized by the presence of circulating plasma cells. PCL can either originate de novo (pPCL) or as secondary PCL (sPCL) in patients with relapsed/refractory multiple myeloma (MM). PCL has a more aggressive clinical presentation than MM with a more frequent extramedullary involvement, such as leptomeningeal infiltration. However, because of the low incidence of this entity, most clinical data come from small retrospective studies. Classical diagnosis criteria of PCL are today under review and the incidence of leptomeningeal infiltration is unknown.
Aims
We aimed to study the clinical features with special emphasis in the incidence leptomeningeal infiltration in patients diagnosed with PCL in our centre.
Methods
Results
Seventeen patients with PCL were included. Six (35.3%) were pPCL and eleven (64.7%) sPCL. Median age at diagnosis was 57 years (range 35-78) and 8 (47.1%) were males. Clinical and analytical features at the moment of diagnosis are recorded in Table 1. Five (29.4%) patients presented with leptomeningeal infiltration; in three of them it was diagnosed at the time of the diagnosis of PCL. All the patients had neurological features. Thirteen (76.4%) patients were able to start a curative treatment: VD in 7 (53.8%) patients, VTD in 2 (15.4%), VAD in 1 (7.7%), D-PACE in 1, MTX-ARAC in 1 patient and RD in the remaining one. Three patients received intrathecal treatment. The intention-to-treat response was: 2 (15.4%) CR, 2 PR, 7 (53.9%) refractory disease/progression and 2 non-evaluable. Only 2 (15.4%) patients achieved enough response (2 CR) to undergo an autologous stem cell transplant (ACST) and only 1 to undergo an allogenic-SCT. With a median follow up of 4 months for all the patients inclosed, median of PFS was 3 (CI 95% 0.47-4.76) months and median of OS was 4 (IC 95% 0.47-7.53) months.
Conclusion
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Plasma cells