

Contributions
Abstract: PB1994
Type: Publication Only
Background
While hematopoietic malignancies are found at increased rates in individuals with acquired immunodeficiency syndrome (AIDS), coincidence of multiple myeloma (MM) and human immunodeficiency virus (HIV) is less common, leading to a paucity of expertise in the treatment of individuals with these co-morbid conditions. Prior to the advent of highly active anti-retroviral therapy (HAART), autologous stem cell transplant (ASCT) was relatively contraindicated for MM patients with HIV due to issues associated with stem cell harvest and the risk of opportunistic infections. With the widespread use of HAART for control of HIV, high dose chemotherapy and ASCT is now the preferred treatment for relapsed lymphoma, the leading hematopoietic malignancy associated with HIV/AIDS. It stands to reason that MM patients with HIV on HAART may benefit equally from aggressive combination treatment of chemotherapy and ASCT.
Aims
This study seeks to evaluate the clinical course and treatment outcomes of patients with HIV and MM treated with high dose therapy and ASCT.
Methods
A single center retrospective case-series study was performed. Data from patients who were HIV-positive and on HAART undergoing ASCT for treatment of MM between January 2000 and June 2016 were collected and analyzed.
Results
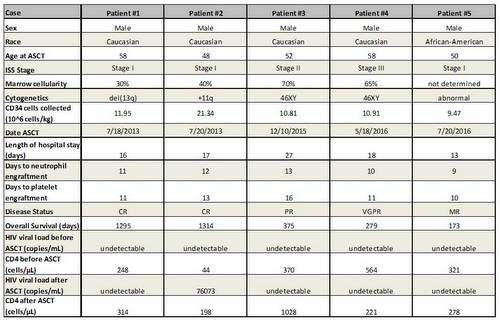
The following table lists patient characteristics. All were male with average age 53.2 years. All were diagnosed with HIV prior to diagnosis of MM and were appropriately treated with HAART prior to ASCT. All patients had undetectable HIV viral titer prior to ASCT, and most remained undetectable after ASCT. Four of five patients had CD4 >200/uL and one patient had CD4 <50/uL prior to ASCT; however all patients recovered CD4 counts after ASCT (and most with improved CD4 count). Adequate CD34(+) stem cells were collected. Patients received high dose melphalan (200 mg/m2) followed by ASCT. HAART was continued during ASCT. Patients experienced usual ASCT toxicities including diarrhea, mucositis, and neutropenic fever. One patient developed sepsis and small bowel obstruction, which resolved with antibiotics and conservative management. All patients had normal neutrophil and platelet engraftments. Post ASCT responses were complete remission (2 patients), very good partial remission (1), partial remission (1) and minimal response (1). All patients are currently alive without relapse or progression 1-4 years from ASCT and receiving post ASCT maintenance with lenalidomide.
Conclusion
Multiple myeloma patients with concurrent HIV infection that is controlled on HAART tolerate ASCT for treatment of myeloma as well as myeloma patients without HIV infection and have generally good outcomes.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Multiple Myeloma, HIV, Autologous hematopoietic stem cell transplantation
Abstract: PB1994
Type: Publication Only
Background
While hematopoietic malignancies are found at increased rates in individuals with acquired immunodeficiency syndrome (AIDS), coincidence of multiple myeloma (MM) and human immunodeficiency virus (HIV) is less common, leading to a paucity of expertise in the treatment of individuals with these co-morbid conditions. Prior to the advent of highly active anti-retroviral therapy (HAART), autologous stem cell transplant (ASCT) was relatively contraindicated for MM patients with HIV due to issues associated with stem cell harvest and the risk of opportunistic infections. With the widespread use of HAART for control of HIV, high dose chemotherapy and ASCT is now the preferred treatment for relapsed lymphoma, the leading hematopoietic malignancy associated with HIV/AIDS. It stands to reason that MM patients with HIV on HAART may benefit equally from aggressive combination treatment of chemotherapy and ASCT.
Aims
This study seeks to evaluate the clinical course and treatment outcomes of patients with HIV and MM treated with high dose therapy and ASCT.
Methods
A single center retrospective case-series study was performed. Data from patients who were HIV-positive and on HAART undergoing ASCT for treatment of MM between January 2000 and June 2016 were collected and analyzed.
Results
The following table lists patient characteristics. All were male with average age 53.2 years. All were diagnosed with HIV prior to diagnosis of MM and were appropriately treated with HAART prior to ASCT. All patients had undetectable HIV viral titer prior to ASCT, and most remained undetectable after ASCT. Four of five patients had CD4 >200/uL and one patient had CD4 <50/uL prior to ASCT; however all patients recovered CD4 counts after ASCT (and most with improved CD4 count). Adequate CD34(+) stem cells were collected. Patients received high dose melphalan (200 mg/m2) followed by ASCT. HAART was continued during ASCT. Patients experienced usual ASCT toxicities including diarrhea, mucositis, and neutropenic fever. One patient developed sepsis and small bowel obstruction, which resolved with antibiotics and conservative management. All patients had normal neutrophil and platelet engraftments. Post ASCT responses were complete remission (2 patients), very good partial remission (1), partial remission (1) and minimal response (1). All patients are currently alive without relapse or progression 1-4 years from ASCT and receiving post ASCT maintenance with lenalidomide.
Conclusion
Multiple myeloma patients with concurrent HIV infection that is controlled on HAART tolerate ASCT for treatment of myeloma as well as myeloma patients without HIV infection and have generally good outcomes.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Multiple Myeloma, HIV, Autologous hematopoietic stem cell transplantation