

Contributions
Abstract: PB1986
Type: Publication Only
Background
MM-003 study has presented a median PFS of 4.0 months and median OS was 13.1 months overall for Pomalidomide and low doses of dexamethasone in RRMM patients. Those results were better when a third drug was added (Poma-Dexa, Poma-Cyclophosphamide-dexa, and Poma-Bortezomib-dexa, ORR 38.9, 64.7 and 85%; PFS 4.4, 9.5, 10.7 months respectively).
Aims
To evaluate the response at therapy with pomalidomide plus dexamethasone in RRMM, and to analyze the efficacy of another drug in high risk MM.
Methods
we reported the clinical experience of the 8 patients treated with pomalidomide and dexamethasone. In patients with high risk MM (cytogenetic, extramedullary myeloma or plasmatic cell leukemia) pomalidomide and dexamethasone have had poor response. In those cases, we have added a third drug (cyclophosphamide or Bortezomib) and we have obtained the best results.
Results
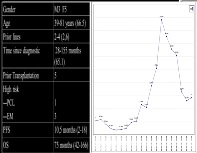
we have used pomalidomide and dexamethasone in 4 patients and poma-dexa-cyclophosphamide in 3 patients (extramedullary myeloma) and poma-bortezomid-dexa in 1 PCL patient. Table1. Demographic characteristic`s patients. Figure1. Response of monoclonal spike.
Conclusion
pomalidomide, dexamethasone and a third drug (cyclophosphamide or Bortezomib) obtain best results (PFS and OS) in high risk RRMM patients. We have not reported more toxicity adding a third drug. In our experience, the response of the extramedullary myeloma with pomalidomide´s triplets is a great option.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Imids
Abstract: PB1986
Type: Publication Only
Background
MM-003 study has presented a median PFS of 4.0 months and median OS was 13.1 months overall for Pomalidomide and low doses of dexamethasone in RRMM patients. Those results were better when a third drug was added (Poma-Dexa, Poma-Cyclophosphamide-dexa, and Poma-Bortezomib-dexa, ORR 38.9, 64.7 and 85%; PFS 4.4, 9.5, 10.7 months respectively).
Aims
To evaluate the response at therapy with pomalidomide plus dexamethasone in RRMM, and to analyze the efficacy of another drug in high risk MM.
Methods
we reported the clinical experience of the 8 patients treated with pomalidomide and dexamethasone. In patients with high risk MM (cytogenetic, extramedullary myeloma or plasmatic cell leukemia) pomalidomide and dexamethasone have had poor response. In those cases, we have added a third drug (cyclophosphamide or Bortezomib) and we have obtained the best results.
Results
we have used pomalidomide and dexamethasone in 4 patients and poma-dexa-cyclophosphamide in 3 patients (extramedullary myeloma) and poma-bortezomid-dexa in 1 PCL patient. Table1. Demographic characteristic`s patients. Figure1. Response of monoclonal spike.
Conclusion
pomalidomide, dexamethasone and a third drug (cyclophosphamide or Bortezomib) obtain best results (PFS and OS) in high risk RRMM patients. We have not reported more toxicity adding a third drug. In our experience, the response of the extramedullary myeloma with pomalidomide´s triplets is a great option.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Imids