

Contributions
Abstract: PB1978
Type: Publication Only
Background
Central nervous system (CNS) propagation is a rare event in multiple myeloma (MM), but may become more prevalent as newer treatment options allow patients to have a prolonged life expectancy and with this comes the selection of increasingly aggressive clones.
Aims
We reviewed 12 MM cases with CNS involvement treated in two hospitals.
Methods
Statistical analyses were performed using the SPSS (version 20.0) software package.
Results
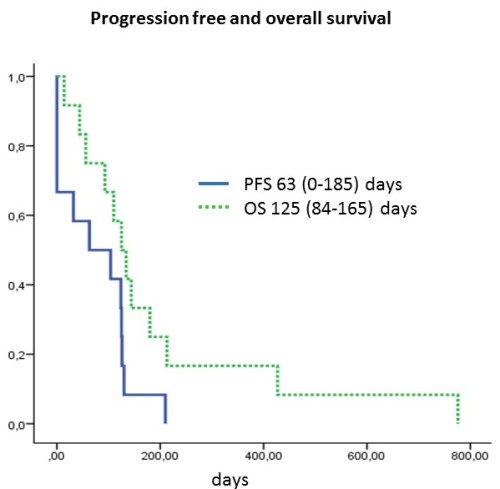
Between 2008 and 2015 twelve MM patient developed CNS involvement which presented in all cases at relapse. The median age at diagnosis and at CNS presentation were 55.5 and 57.4 years. At first presentation nine had ISS 3, one ISS 2 and two ISS 1 stage disease, two patient presented originally as plasma cell leukaemia. FISH showed 1q amplification in 4, 13q deletion in 4, translocation (4;14) in 1, t(11;14) together with 17p deletion in 1, hyperdiploidity in 1 and complex karyotype in 2 cases. In 2 cases we demonstrated the development of new karyotypic abnormalities (one 1q amplification, one 17p deletion) at CNS progression. The median number of treatment lines prior to CNS progression was 2 which included bortezomib in all and thalidomide in all but one cases, two patients had lenalidomide. Six patients had ASCT before the CNS progression from which one had a second ASCT and one a reduced intensity allogeneic transplantation. The median time from diagnosis to CNS progression was 23.9 (3-65) months. Eight patients presented with cerebral nerve palsy, 2 with paraplegia, 1 with hypacusis and 1 with headache. CSF cytospin or flow cytometry was positive in 7, MRI or CT supported the diagnosis in 4 patients. Treatment consisted of combination chemotherapy, intrathecal chemotherapy, cranio-caudal radiotherapy and imids with various success. The PFS and OS from CNS progression was 63 and 125 days. Two patients survived for over a year (427 and 776 days), both responded in terms of CNS symptoms to imid-based combination therapy and one had cranio-caudal radiotherapy.
Conclusion
CNS progression in MM has a particularly poor prognosis as it represents a late stage of an aggressive relapse which often shows chemo-refractoriness. The differential diagnosis includes infection, autoimmune or vascular diseases of the CNS as well as paraneoplasia and drug toxicity. The CNS penetration of the effective myeloma drugs is poor except for the imids, and drugs with CNS availability are usually not very effective in refractory MM.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Myeloma, CNS
Abstract: PB1978
Type: Publication Only
Background
Central nervous system (CNS) propagation is a rare event in multiple myeloma (MM), but may become more prevalent as newer treatment options allow patients to have a prolonged life expectancy and with this comes the selection of increasingly aggressive clones.
Aims
We reviewed 12 MM cases with CNS involvement treated in two hospitals.
Methods
Statistical analyses were performed using the SPSS (version 20.0) software package.
Results
Between 2008 and 2015 twelve MM patient developed CNS involvement which presented in all cases at relapse. The median age at diagnosis and at CNS presentation were 55.5 and 57.4 years. At first presentation nine had ISS 3, one ISS 2 and two ISS 1 stage disease, two patient presented originally as plasma cell leukaemia. FISH showed 1q amplification in 4, 13q deletion in 4, translocation (4;14) in 1, t(11;14) together with 17p deletion in 1, hyperdiploidity in 1 and complex karyotype in 2 cases. In 2 cases we demonstrated the development of new karyotypic abnormalities (one 1q amplification, one 17p deletion) at CNS progression. The median number of treatment lines prior to CNS progression was 2 which included bortezomib in all and thalidomide in all but one cases, two patients had lenalidomide. Six patients had ASCT before the CNS progression from which one had a second ASCT and one a reduced intensity allogeneic transplantation. The median time from diagnosis to CNS progression was 23.9 (3-65) months. Eight patients presented with cerebral nerve palsy, 2 with paraplegia, 1 with hypacusis and 1 with headache. CSF cytospin or flow cytometry was positive in 7, MRI or CT supported the diagnosis in 4 patients. Treatment consisted of combination chemotherapy, intrathecal chemotherapy, cranio-caudal radiotherapy and imids with various success. The PFS and OS from CNS progression was 63 and 125 days. Two patients survived for over a year (427 and 776 days), both responded in terms of CNS symptoms to imid-based combination therapy and one had cranio-caudal radiotherapy.
Conclusion
CNS progression in MM has a particularly poor prognosis as it represents a late stage of an aggressive relapse which often shows chemo-refractoriness. The differential diagnosis includes infection, autoimmune or vascular diseases of the CNS as well as paraneoplasia and drug toxicity. The CNS penetration of the effective myeloma drugs is poor except for the imids, and drugs with CNS availability are usually not very effective in refractory MM.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Myeloma, CNS