
LACK OF CD56 EXPRESSION IN MULTIPLE MYELOMA PATIENTS WITH RISS 2 DISEASE IS ASSOCIATED WITH WORSE PROGNOSIS AND ABOLISHED WITH AUTOLOGOUS STEM CELL TRANSPLANTATION
(Abstract release date: 05/18/17)
EHA Library. Skerget M. 05/18/17; 182679; PB1965

Matevz Skerget
Contributions
Contributions
Abstract
Abstract: PB1965
Type: Publication Only
Background
Multiple myeloma (MM) is a hematologic disease in which accumulation of malignant plasma cells and high levels of monoclonal protein and free light chains lead to bone marrow failure, hypercalcemia, lytic bone lesions and renal failure. Myeloma cells are distinguished from normal plasma cells by an aberrant immunophenotype. They express CD56, which is present in 70-80 % and can be used to distinguish myeloma cells by flow cytometry. The expression of CD56 is constant throughout the course of the disease. The lack of CD56 expression in myeloma cells decreases the adherence of myeloma cells to the cell matrix and is associated with higher levels of bone marrow infiltration and peripheral blood involvement, higher incidence of extramedullary disease, renal insufficiency, Bence Jones protein, plasma cell leukemia and t(11;14). The lack of CD117 expression is associated with higher levels of bone marrow infiltration, renal impairment, elevated β2-microglobulin and cytogenetic aberrations including t(11;14), t(4;14) and del(13q). CD28 expression is present in 15 – 45 % of patients and is associated with unfavorably cytogenetic changes including t(4;14) and del(17p) and shorter PFS and OS despite aHSCT.
Aims
Aim of our retrospective study was to evaluate the impact of CD56, CD117 and CD28 expression on clinical characteristics and PFS in newly diagnosed MM patients treated with bortezomib based induction therapy.
Methods
We retrospectively analyzed 110 newly diagnosed MM patients from our national registry that had data available at the time of diagnosis. Immunophenotype was determined using a panel consisting of CD19/CD38/CD45/CD56/CD138 to distinguish and to enumerate MM cells. Monoclonal antibodies directed against CD20, CD28, and CD117 were used additionally. All samples were routinely tested for the presence of recurrent chromosomal aberrations, i.e. del 1p, amp1q, del6q, amp15q, del13, del17, t(4;14), t(14;16) and t(11;14) using commercially available DNA probes.
Results
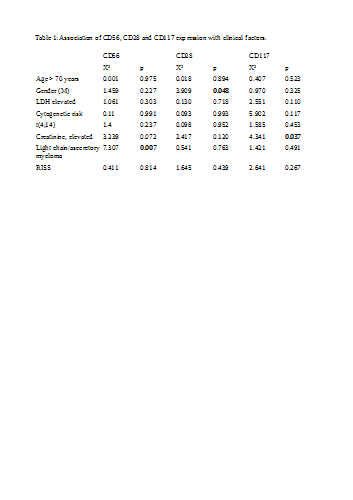
We found no association between CD56 expression and age, gender, elevated LDH, cytogenetic risk or RISS stage. We found a strong association between lack of CD56 expression and light-chain only or asecretory myeloma. There was an association between CD28 expression and female gender (Table 1). In multivariate analysis including age, elevated creatinine, RISS, aHSCT, CD28, CD56 and CD117 expression, CD56 expression was associated with a 47 % reduced hazard for progression (Exp(B) = 0.527, p = 0.03). Other factors with statistically significant impact on progression were aHSCT and age.
In patients not undergoing aHSCT lacking CD56 expression in comparison to those with an aberrant CD56 expression, the difference in PFS was statistically significant with a PFS of 8 vs 18 Month (Log Rank p = 0.088, Breslow p = 0.046). When stratified according to RISS stage, only patients in stage 2 disease had a significant reduction in PFS with lack of CD56 expression.
Conclusion
CD56 expression was prognostic for PFS only in the patient cohort not undergoing aHSCT. As previously reported aHSCT seems to abrogate the negative impact of CD56 negativity. We propose CD56 expression to be used as a prognostic marker in patients with RISS 2 stage disease and when possible these patients should undergo aHSCT.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Myeloma, Immunophenotype, CD56, Autologous hematopoietic stem cell transplantation
Abstract: PB1965
Type: Publication Only
Background
Multiple myeloma (MM) is a hematologic disease in which accumulation of malignant plasma cells and high levels of monoclonal protein and free light chains lead to bone marrow failure, hypercalcemia, lytic bone lesions and renal failure. Myeloma cells are distinguished from normal plasma cells by an aberrant immunophenotype. They express CD56, which is present in 70-80 % and can be used to distinguish myeloma cells by flow cytometry. The expression of CD56 is constant throughout the course of the disease. The lack of CD56 expression in myeloma cells decreases the adherence of myeloma cells to the cell matrix and is associated with higher levels of bone marrow infiltration and peripheral blood involvement, higher incidence of extramedullary disease, renal insufficiency, Bence Jones protein, plasma cell leukemia and t(11;14). The lack of CD117 expression is associated with higher levels of bone marrow infiltration, renal impairment, elevated β2-microglobulin and cytogenetic aberrations including t(11;14), t(4;14) and del(13q). CD28 expression is present in 15 – 45 % of patients and is associated with unfavorably cytogenetic changes including t(4;14) and del(17p) and shorter PFS and OS despite aHSCT.
Aims
Aim of our retrospective study was to evaluate the impact of CD56, CD117 and CD28 expression on clinical characteristics and PFS in newly diagnosed MM patients treated with bortezomib based induction therapy.
Methods
We retrospectively analyzed 110 newly diagnosed MM patients from our national registry that had data available at the time of diagnosis. Immunophenotype was determined using a panel consisting of CD19/CD38/CD45/CD56/CD138 to distinguish and to enumerate MM cells. Monoclonal antibodies directed against CD20, CD28, and CD117 were used additionally. All samples were routinely tested for the presence of recurrent chromosomal aberrations, i.e. del 1p, amp1q, del6q, amp15q, del13, del17, t(4;14), t(14;16) and t(11;14) using commercially available DNA probes.
Results
We found no association between CD56 expression and age, gender, elevated LDH, cytogenetic risk or RISS stage. We found a strong association between lack of CD56 expression and light-chain only or asecretory myeloma. There was an association between CD28 expression and female gender (Table 1). In multivariate analysis including age, elevated creatinine, RISS, aHSCT, CD28, CD56 and CD117 expression, CD56 expression was associated with a 47 % reduced hazard for progression (Exp(B) = 0.527, p = 0.03). Other factors with statistically significant impact on progression were aHSCT and age.
In patients not undergoing aHSCT lacking CD56 expression in comparison to those with an aberrant CD56 expression, the difference in PFS was statistically significant with a PFS of 8 vs 18 Month (Log Rank p = 0.088, Breslow p = 0.046). When stratified according to RISS stage, only patients in stage 2 disease had a significant reduction in PFS with lack of CD56 expression.
Conclusion
CD56 expression was prognostic for PFS only in the patient cohort not undergoing aHSCT. As previously reported aHSCT seems to abrogate the negative impact of CD56 negativity. We propose CD56 expression to be used as a prognostic marker in patients with RISS 2 stage disease and when possible these patients should undergo aHSCT.
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Myeloma, Immunophenotype, CD56, Autologous hematopoietic stem cell transplantation
{{ help_message }}
{{filter}}