

Contributions
Abstract: PB1963
Type: Publication Only
Background
A solitary plasmacytoma (SP) is a rare neoplastic mass of monoclonal plasma cells that can either be localized in bone (solitary plasmacytoma of bone, SPB), or soft tissue (extramedullary plasmacytoma, EMP), without evidence of multiple myeloma (MM). The median age at diagnosis is 65 years. Some patients present a monoclonal band (MB) at diagnosis, and a proportion progresses to MM. The low incidence of this entity has prevented reaching definite conclusions with regards to prognostic factors and treatment.
Aims
In this study we retrospectively analysed the clinical presentation, treatment and outcome of all patients with SP treated in our centre in order to establish relevant prognostic clinical features and management options.
Methods
Between 1985 and 2016, 27 patients with SP (20 SPB, 7 EMP) were treated in Ramon y Cajal Hospital (Madrid), with a median follow up of 8 years. The time to relapse, progression to MM or death was measured in months. The progression free survival (PFS) and overall survival (OS) were estimated using the Kaplan-Meier method. The comparison of PFS/OS was performed using the Log Rank test. Student´s T test was used to compare the average age at diagnosis. To determine the association between the presence of MB or the subtype of SP, and progression to MM, we used Fisher’s exact test. All statistical analysis was performed with the software SPSS 24.0.
Results
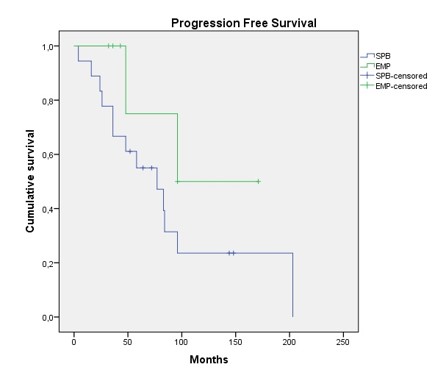
The average age at diagnosis was 56 years (±18): 51 (±17) for SPB, and 72 (±5) for EMP (p<0.05), with a male:female ratio of 2.4:1. The most frequent location was the axial skeleton (80%) for SPB, and the airway in the case of EMP (57%). In most cases, the initial symptom of SPB had been pain (45%), and local discomfort for EMP. 52% of patients presented a MB at diagnosis, without significant differences between subgroups. With regards to treatment, combined therapy was the preferred option in the case of SPB (60%), whereas unimodal treatment strategies were more frequently used in EMP (86%). 11 of the 20 patients with SPB progressed to MM (55%) in a median time of 4 years, while none of the patients with EMP progressed (p<0.05). The 5 year PFS and OS was 61% and 90% respectively, 31% and 74% at 10 years. Although a tendency towards a higher PFE was observed in the EMP group, it was not statistically significant. No differences were found in PFS/OS between age groups (<60 or ≥60 years), axial vs appendicular skeleton location in SBP, type of treatment received, or the presence of MB. Furthermore, no association was found between the presence of MB at diagnosis and progression to MM.
Conclusion
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Plasma cells
Abstract: PB1963
Type: Publication Only
Background
A solitary plasmacytoma (SP) is a rare neoplastic mass of monoclonal plasma cells that can either be localized in bone (solitary plasmacytoma of bone, SPB), or soft tissue (extramedullary plasmacytoma, EMP), without evidence of multiple myeloma (MM). The median age at diagnosis is 65 years. Some patients present a monoclonal band (MB) at diagnosis, and a proportion progresses to MM. The low incidence of this entity has prevented reaching definite conclusions with regards to prognostic factors and treatment.
Aims
In this study we retrospectively analysed the clinical presentation, treatment and outcome of all patients with SP treated in our centre in order to establish relevant prognostic clinical features and management options.
Methods
Between 1985 and 2016, 27 patients with SP (20 SPB, 7 EMP) were treated in Ramon y Cajal Hospital (Madrid), with a median follow up of 8 years. The time to relapse, progression to MM or death was measured in months. The progression free survival (PFS) and overall survival (OS) were estimated using the Kaplan-Meier method. The comparison of PFS/OS was performed using the Log Rank test. Student´s T test was used to compare the average age at diagnosis. To determine the association between the presence of MB or the subtype of SP, and progression to MM, we used Fisher’s exact test. All statistical analysis was performed with the software SPSS 24.0.
Results
The average age at diagnosis was 56 years (±18): 51 (±17) for SPB, and 72 (±5) for EMP (p<0.05), with a male:female ratio of 2.4:1. The most frequent location was the axial skeleton (80%) for SPB, and the airway in the case of EMP (57%). In most cases, the initial symptom of SPB had been pain (45%), and local discomfort for EMP. 52% of patients presented a MB at diagnosis, without significant differences between subgroups. With regards to treatment, combined therapy was the preferred option in the case of SPB (60%), whereas unimodal treatment strategies were more frequently used in EMP (86%). 11 of the 20 patients with SPB progressed to MM (55%) in a median time of 4 years, while none of the patients with EMP progressed (p<0.05). The 5 year PFS and OS was 61% and 90% respectively, 31% and 74% at 10 years. Although a tendency towards a higher PFE was observed in the EMP group, it was not statistically significant. No differences were found in PFS/OS between age groups (<60 or ≥60 years), axial vs appendicular skeleton location in SBP, type of treatment received, or the presence of MB. Furthermore, no association was found between the presence of MB at diagnosis and progression to MM.
Conclusion
Session topic: 14. Myeloma and other monoclonal gammopathies - Clinical
Keyword(s): Plasma cells