

Contributions
Abstract: PB1891
Type: Publication Only
Background
In recent years the incidence of multi-resistant bacteria (MRB) infections have notably increase. These infections are especially serious in hematological patients because of the immunosupression derived from their illness and their treatments. This increase is related to a high mortality rate and high health costs due to the severity of the infections and the difficulty in setting adequate therapy due to the lack of new antibiotics against these pathogens.
Aims
Define the MRB infections incidence and ways of presentation. As a secondary goal we try to determine if the isolation of these MRB has affected our empiric antibiotic therapy decision.
Methods
We retrospectively collected all positive blood stream cultures from hematologic patients from January 2012 to December 2016. We studied the characteristics, clinical features and pathogen isolates of our patients when the blood cultures were obtained.
Results
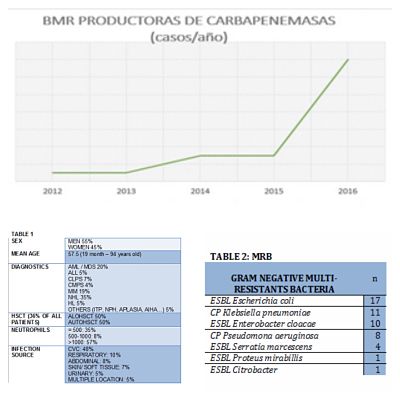
1005 positive blood stream cultures were collected in 382 patients. The main characteristics of the patients are shown on table 1. The infection source was: central venous catheter (CVC) in 48% of patients (including tunneled, non-tunneled and PICC lines), respiratory 10%, abdominal 8%, urinary 5%, skin/soft tissue 7% and multiple location 5%. Regarding CVC isolation's, 11% were interpreted as contamination and 6% as colonization.
Conclusion
- Current antimicrobial resistance, especially concerning G- in our study, is particularly worrisome due to development of resistance to all available antimicrobial agents. The incidence of multi-resistant G+ is not very high.
Session topic: 29. Infectious diseases, supportive care
Abstract: PB1891
Type: Publication Only
Background
In recent years the incidence of multi-resistant bacteria (MRB) infections have notably increase. These infections are especially serious in hematological patients because of the immunosupression derived from their illness and their treatments. This increase is related to a high mortality rate and high health costs due to the severity of the infections and the difficulty in setting adequate therapy due to the lack of new antibiotics against these pathogens.
Aims
Define the MRB infections incidence and ways of presentation. As a secondary goal we try to determine if the isolation of these MRB has affected our empiric antibiotic therapy decision.
Methods
We retrospectively collected all positive blood stream cultures from hematologic patients from January 2012 to December 2016. We studied the characteristics, clinical features and pathogen isolates of our patients when the blood cultures were obtained.
Results
1005 positive blood stream cultures were collected in 382 patients. The main characteristics of the patients are shown on table 1. The infection source was: central venous catheter (CVC) in 48% of patients (including tunneled, non-tunneled and PICC lines), respiratory 10%, abdominal 8%, urinary 5%, skin/soft tissue 7% and multiple location 5%. Regarding CVC isolation's, 11% were interpreted as contamination and 6% as colonization.
Conclusion
- Current antimicrobial resistance, especially concerning G- in our study, is particularly worrisome due to development of resistance to all available antimicrobial agents. The incidence of multi-resistant G+ is not very high.
Session topic: 29. Infectious diseases, supportive care