

Contributions
Abstract: PB1867
Type: Publication Only
Background
Efficacy of PD-1 (programmed death-1) inhibitors in relapsed/refractory Hodgkin lymphoma (HL) has been established, but their role in relapse after allogeneic stem cell transplant (alloSCT) remains controversial due to the perceived risk of exacerbating graft-versus-host disease (GVHD). The literature is largely limited to case reports in patients with no or quiescent GVHD.
Aims
To describe the outcome of PD-1 inhibitor therapy and subsequent management in patients with concomitant biopsy proven active GVHD and progressive HL after alloSCT.
Methods
We describe the treatment and management of two patients in our centre.
Results
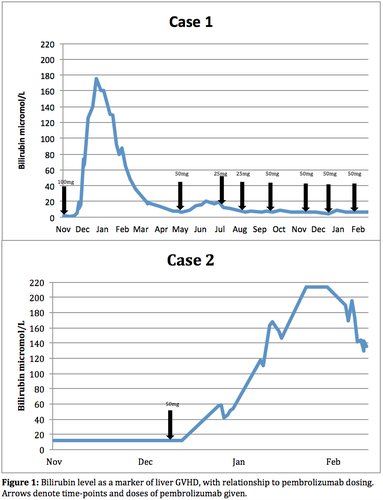
Case 1 had both extensive bony, lung and nodal HL with active skin, pleuropericardial and liver GVHD 6 months after donor leucocyte infusion (DLI) and immunosuppression withdrawal and 24 months after sibling alloHSCT. Fifty % of the standard pembrolizumab dose (100mg) produced a PET partial response after 5 weeks but with concomitant biopsy proven, severe exacerbation of liver GHVD. The latter was managed with prednisolone, everolimus, ursodeoxycholic acid (UDCA) and subsequently tacrolimus with gradual but substantial improvement in liver function over the next 5 months (Figure 1) in the absence of further PD-1 blockade, but with progression of lymphoma. Pembrolizumab 50mg was then given with lymphoma response but again a significant (but less severe) flare of liver GVHD occurred. Subsequent 25mg doses failed to prevent lymphoma progression. Reintroduction of 50mg doses approximately each 6 weeks for 4 doses with prophylactic everolimus, low dose prednisolone and ruxolitinib, has resulted in ongoing substantial but incomplete PET responses with associated stable liver GHVD.
Conclusion
PD-1 inhibitors can exert powerful graft vs HL effects even in patients with progression in the context of active GVHD, but at the expense of substantial GVHD exacerbation. Further exploration of approaches such as individualised dose titration according to response and GVHD activity and prophylactic therapy with non-calcineurin based immunosuppression which may not mitigate the anti-lymphoma effect will help evaluate whether durable responses with tolerable toxicity is possible in this context.
Session topic: 17. Hodgkin lymphoma - Clinical
Keyword(s): Immunotherapy, Hodgkin's Lymphoma, Graft-versus-host disease (GVHD)
Abstract: PB1867
Type: Publication Only
Background
Efficacy of PD-1 (programmed death-1) inhibitors in relapsed/refractory Hodgkin lymphoma (HL) has been established, but their role in relapse after allogeneic stem cell transplant (alloSCT) remains controversial due to the perceived risk of exacerbating graft-versus-host disease (GVHD). The literature is largely limited to case reports in patients with no or quiescent GVHD.
Aims
To describe the outcome of PD-1 inhibitor therapy and subsequent management in patients with concomitant biopsy proven active GVHD and progressive HL after alloSCT.
Methods
We describe the treatment and management of two patients in our centre.
Results
Case 1 had both extensive bony, lung and nodal HL with active skin, pleuropericardial and liver GVHD 6 months after donor leucocyte infusion (DLI) and immunosuppression withdrawal and 24 months after sibling alloHSCT. Fifty % of the standard pembrolizumab dose (100mg) produced a PET partial response after 5 weeks but with concomitant biopsy proven, severe exacerbation of liver GHVD. The latter was managed with prednisolone, everolimus, ursodeoxycholic acid (UDCA) and subsequently tacrolimus with gradual but substantial improvement in liver function over the next 5 months (Figure 1) in the absence of further PD-1 blockade, but with progression of lymphoma. Pembrolizumab 50mg was then given with lymphoma response but again a significant (but less severe) flare of liver GVHD occurred. Subsequent 25mg doses failed to prevent lymphoma progression. Reintroduction of 50mg doses approximately each 6 weeks for 4 doses with prophylactic everolimus, low dose prednisolone and ruxolitinib, has resulted in ongoing substantial but incomplete PET responses with associated stable liver GHVD.
Conclusion
PD-1 inhibitors can exert powerful graft vs HL effects even in patients with progression in the context of active GVHD, but at the expense of substantial GVHD exacerbation. Further exploration of approaches such as individualised dose titration according to response and GVHD activity and prophylactic therapy with non-calcineurin based immunosuppression which may not mitigate the anti-lymphoma effect will help evaluate whether durable responses with tolerable toxicity is possible in this context.
Session topic: 17. Hodgkin lymphoma - Clinical
Keyword(s): Immunotherapy, Hodgkin's Lymphoma, Graft-versus-host disease (GVHD)