

Contributions
Abstract: PB1844
Type: Publication Only
Background
In the Western hemisphere, Gaucher disease (GD) type 1 is the most common GD phenotype, but the prevalence of GD type 3 is increasing. The spectrum of signs and symptoms of the different GD phenotypes ranges from fatal perinatal to asymptomatic adult disease, and the heterogeneity of its presentation contributes to both misdiagnosis and delays in diagnosis by clinicians unfamiliar with the disease. The Gaucher Earlier Diagnosis Consensus (GED-C) Delphi initiative determined which signs and patient co-variables are regarded by experts in GD as most indicative of GD types 1 or 3 in the early stages.
Aims
From the findings of the GED-C expert consensus, to generate a simple web-based point-scoring system (PSS) suitable for use across clinical specialties, that provides guidance based on patients’ presenting signs as to whether GD diagnostic testing is appropriate.
Methods
An anonymous three-round Delphi process, conducted among a global panel of 22 expert physicians, established consensus on which signs and co-variables may be important in early GD type 1 and, separately, in early GD type 3. In round 1, free-text responses provided by the panel were categorized by an independent administrator. This categorization was checked and consolidated into summary factors by the non-voting co-chairs. In round 2, the factors were rated for importance by the panel using a 5-point Likert scale (1 = not important, 3 = important, 5 = extremely important). Any factors assigned an importance score of ≥ 3 by > 75% of respondents were then rated for agreement in round 3, using a 5-point pivoted Likert scale (1 = strongly disagree, 3 = neither agree nor disagree, 5 = strongly agree). Consensus was defined as a score of ≥ 4 by > 67% of respondents. Factors meeting this threshold were classified as major; all other factors were classified as minor. The co-chairs defined value ranges corresponding to mild, moderate or severe forms of five of the major signs of GD (anaemia, hepatomegaly, hyperferritinaemia, splenomegaly and thrombocytopenia). Panel members indicated whether they regarded each range as consistent with a GD diagnosis. This information was used in combination with the classifications of signs and co-variables as major or minor to create a prototype PSS.
Results
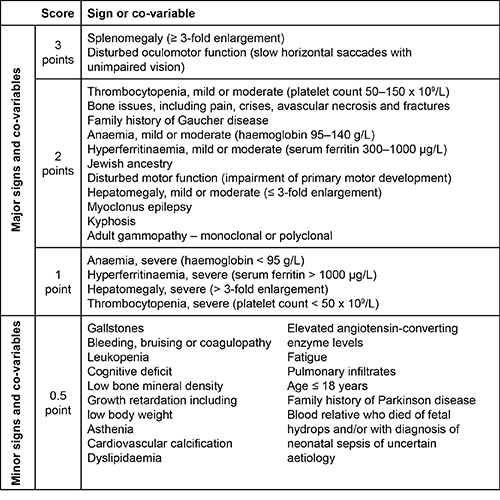
There was a 100% response rate in each round. Factors identified as major or minor in GD types 1 or 3 are given in the table. There was 100% agreement that splenomegaly (≥ 3-fold enlargement) and disturbed oculomotor function (slow horizontal saccades with unimpaired vision) are major signs in GD, and these were assigned a score of 3 in the prototype PSS; other major signs and co-variables were assigned a score of 2. The panel was divided about whether severe anaemia, hepatomegaly, hyperferritinaemia and severe thrombocytopenia were consistent with a GD diagnosis, so these were assigned a score of 1. All minor signs and co-variables were assigned a score of 0.5.
Conclusion
A prototype PSS to inform GD diagnostic testing has been developed from the GED-C Delphi initiative. The PSS will be validated with retrospective patient data. Total patient scores based on presenting signs and co-variables will be used to determine empirically a minimum threshold score that captures positive tests for GD. Abstract submitted on behalf of the GED-C panel and the EHA Scientific Working Group ‘Quality of Life and Symptoms’. Administration of the GED-C initiative was funded by unrestricted educational grants from Shire International GmbH.
Session topic: 27. Enzymopathies, membranopathies and other anemias
Keyword(s): Gaucher disease, Ferritin, Thrombocytopenia, Spleen
Abstract: PB1844
Type: Publication Only
Background
In the Western hemisphere, Gaucher disease (GD) type 1 is the most common GD phenotype, but the prevalence of GD type 3 is increasing. The spectrum of signs and symptoms of the different GD phenotypes ranges from fatal perinatal to asymptomatic adult disease, and the heterogeneity of its presentation contributes to both misdiagnosis and delays in diagnosis by clinicians unfamiliar with the disease. The Gaucher Earlier Diagnosis Consensus (GED-C) Delphi initiative determined which signs and patient co-variables are regarded by experts in GD as most indicative of GD types 1 or 3 in the early stages.
Aims
From the findings of the GED-C expert consensus, to generate a simple web-based point-scoring system (PSS) suitable for use across clinical specialties, that provides guidance based on patients’ presenting signs as to whether GD diagnostic testing is appropriate.
Methods
An anonymous three-round Delphi process, conducted among a global panel of 22 expert physicians, established consensus on which signs and co-variables may be important in early GD type 1 and, separately, in early GD type 3. In round 1, free-text responses provided by the panel were categorized by an independent administrator. This categorization was checked and consolidated into summary factors by the non-voting co-chairs. In round 2, the factors were rated for importance by the panel using a 5-point Likert scale (1 = not important, 3 = important, 5 = extremely important). Any factors assigned an importance score of ≥ 3 by > 75% of respondents were then rated for agreement in round 3, using a 5-point pivoted Likert scale (1 = strongly disagree, 3 = neither agree nor disagree, 5 = strongly agree). Consensus was defined as a score of ≥ 4 by > 67% of respondents. Factors meeting this threshold were classified as major; all other factors were classified as minor. The co-chairs defined value ranges corresponding to mild, moderate or severe forms of five of the major signs of GD (anaemia, hepatomegaly, hyperferritinaemia, splenomegaly and thrombocytopenia). Panel members indicated whether they regarded each range as consistent with a GD diagnosis. This information was used in combination with the classifications of signs and co-variables as major or minor to create a prototype PSS.
Results
There was a 100% response rate in each round. Factors identified as major or minor in GD types 1 or 3 are given in the table. There was 100% agreement that splenomegaly (≥ 3-fold enlargement) and disturbed oculomotor function (slow horizontal saccades with unimpaired vision) are major signs in GD, and these were assigned a score of 3 in the prototype PSS; other major signs and co-variables were assigned a score of 2. The panel was divided about whether severe anaemia, hepatomegaly, hyperferritinaemia and severe thrombocytopenia were consistent with a GD diagnosis, so these were assigned a score of 1. All minor signs and co-variables were assigned a score of 0.5.
Conclusion
A prototype PSS to inform GD diagnostic testing has been developed from the GED-C Delphi initiative. The PSS will be validated with retrospective patient data. Total patient scores based on presenting signs and co-variables will be used to determine empirically a minimum threshold score that captures positive tests for GD. Abstract submitted on behalf of the GED-C panel and the EHA Scientific Working Group ‘Quality of Life and Symptoms’. Administration of the GED-C initiative was funded by unrestricted educational grants from Shire International GmbH.
Session topic: 27. Enzymopathies, membranopathies and other anemias
Keyword(s): Gaucher disease, Ferritin, Thrombocytopenia, Spleen